MEDULLOBLASTOMA
•Download as PPTX, PDF•
32 likes•11,123 views

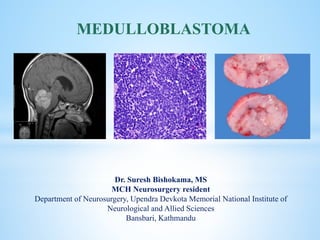
Medulloblastoma- A primitive neuroectodermal tumors (PNETs) is the most common malignant brain tumor of childhood (WHO IV) arising from the vermis in the inferior medullary velum. It comprises up to 18% of all pediatric brain tumors. WNT and Shh pathway plays major role in its pathogenesis. c-erbB-2 (HER2/neu) oncogene expression has prognostic value. Norcantharidin, Vismodegib, Sonidegib are the future in medulloblastoma.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to MEDULLOBLASTOMA
Similar to MEDULLOBLASTOMA (20)
More from suresh Bishokarma
More from suresh Bishokarma (20)
Recently uploaded
Recently uploaded (20)
MEDULLOBLASTOMA
- 1. cka Dr. Suresh Bishokama, MS MCH Neurosurgery resident Department of Neurosurgery, Upendra Devkota Memorial National Institute of Neurological and Allied Sciences Bansbari, Kathmandu MEDULLOBLASTOMA
- 2. Cushing Report: 1930 Coined Medulloblastoma: Bailey and Cushing 1983: PNET HISTORY
- 3. Medulloblastoma is the most common malignant brain tumor of childhood (WHO IV) and comprises up to 18-30% of all pediatric brain tumors. Medulloblastomas are typically midline cerebellar lesions arising from the vermis in the inferior medullary velum; however, in older children and adults they can arise from the cerebellar hemispheres. Medulloblastomas are related to primitive neuroectodermal tumors (PNETs) and occur exclusively in the posterior fossa. INTRODUCTION
- 4. Overall medulloblastomas account for 12-25 % of all pediatric CNS tumors, and 30-40% of pediatric posterior fossa tumors. They are also seen in adults but only account for 0.4-1.0% of adult brain tumor. M:F ratio of 2:1, although this is only true of group 3 and 4 tumors They usually present in childhood with 77% of cases before the age of 19. The median age of diagnosis is 9 years. When diagnosed in adulthood, they typically present in the 3rd and 4th decades and are more likely to arise in atypical locations (see below). When they present in adulthood, there is often a better prognosis. (Younger the poorer) EPIDEMIOLOGY
- 5. N Nitroso compound Vegetables are protective JC virus Genetic conditions: Li-Fraumani, Gorlin, Turcot P53, IGF, c-MYC and N-MYC oncogenic transcription factor, Apoptotic pathway: Bcl-2 ASSOCIATION
- 6. Medulloblastoma to arise from the external granule layer of the developing cerebellum and others have proposed that the cell of origin arises from a subventricular progenitor zone. PATHOGENESIS
- 7. WNT is a ligand for the transmembrane protein FRIZZLED and major cytoplasmic component of the WNT pathway is APC/GSK-3B/AXIN complex. In absence of WNT this complex phosphorylates B catenin, thereby targeting it for degradation. B catenin in nucleus promotes cellular proliferation. WNT PATHWAY
- 8. Sonig Hedge Hog (SHH) Sonig Hedge Hog (SHH) is a diffusible mitogenic protein that binds to the transmembrane receptor protein (PATCHED 1-PTCH1). In the absence of SHH, PTCH1 binds with SMO. This complex inhibit glioma associated oncogene homolog (GLI) and hence cellular proliferation. However, when PTCH1 binds with SHH, inhibitor effect of SMO-PTCH1 complex are reversed leading to activation of GLI and enhanced oncogenesis.
- 9. WNT tumours should be identified by two of the following markers: Nuclear ß-catenin accumulation (IHC) Monosomy 6 (whole chromosome loss) by FISH CTNNB1 mutation WNT pattern by DNA methylation or by gene expression profiling SHH, Group 3 and Group 4 IHC c-myc amplification (FISH) Genome-wide methylation
- 10. Classic : (90%): Undifferentiated cells with hyperchromatic nuclei, (Homer wright rosette suggesting neuronal differentiation, Blue tumor Desmoplastic : (6%): Classic + Glomeruli (pale island of collagen): Least aggressive Nodularity MBEN : Diffuse variant in <3 years child: good prognosis Large cell Anaplastic : (4%): early seed, high mitosis: poor prognosis HISTOLOGICAL SUBTYPES Homer-Wright rosettes composed of neoplastic cells concentrically arranged around fibrillary processes
- 11. Diffuse masses of small, undifferentiated oval or round cells. Some medulloblastomas show neuronal, glial and other differentiation. Nuclear moulding due to compactness inside cell. Neuronal differentiation is manifested by neuropil and rosette formation. Rosettes are groups of tumor cells arranged in a circle around a fibrillary center. Mature neurons may also be found infrequently. Glial differentiation in some tumors is reflected by GFAP-positive cells. There may also be differentiation along oligodendroglial or ependymal lines. CLASSIC MEDULLOBLASTOMA
- 12. Pale nodules are composed uniform round to spindle shaped neuronal-appearing cells which are not as active mitotically as the surrounding darker tumor. They are present within a reticulin-poor fine fibrillary background DESMOPLASTIC MB
- 13. Large cell anaplastic medulloblastoma composed of sheets of highly atypical cells. A focus of necrosis is present just above the center of the image. The tumor cells have irregular hyperchromatic nuclei with nuclear molding and little cytoplasm ANAPLASTIC MB
- 14. Medulloblastoma can spread along cerebrospinal fluid (CSF) pathways and also rarely to systemic sites (bone, lung). Leptomeningeal dissemination constitutes the most common pattern of recurrence for Group 3 and Group 4 patients, and usually leads to a quick progressive clinical decline despite therapy.
- 15. New type: Medulloblastoma NOS. CLINICOPATHOLOGICAL AND MOLECULAR CHARACTERISTICS OF MB SUBGROUPS CLINICOPATHOLOGICALAND MOLECULAR CHARACTERISTICS OF MB SUBGROUP CHARACTER WNT 10% SHH: 25% GP3: 25% GP4: 40%; MC GENDER M=F M=F M>F M>F PEAK AGE Children Children Infants Children OCCURRENCE Arise from foramen of luschka (CP angle) Laterally cerebellar hemisphere, and vermis 4th ventricle 4th ventricle ENHANCEMENT Intensely enhancing like ependymoma but diffusion restriction Intermediate Intermediate Usually non-enhancing HISTOLOGY Classic, rarely LCA Desmoplastic/MBEN, Classic, LCA Classic, LCA Classic, LCA GENE MUTATED CTNNB1, TP53 CTNNB1, TP53, 3q gain, 9p deletion MYC amp, OTX2, SMARCA4 KDM6A, MYCN SNCAIP duplication IHC B-catenin +(including nuclear and cytoplasmic) CTNNB1 mutation, GAB1 (-) Cytoplasmic B-Catenin+; GLI amplification; SMO mutation; MYCN+ GAB1+, YAB1+, PTCH1+, SMO+, P53± MYCN+++; YAB/GAB- Minimal amplification; CDK6+; YAB/GAB (-) METASTASIS Low Extremely low High Frequent PROGNOSIS Best prognosis Intermediate Poor Intermediate
- 16. Molecular group / Immunoreactivity GAB1 ß-catenin YAP1 WNT Negative Nuclear + Cytoplasmic + Nuclear + Cytoplasmic SHH Cytoplasmic Cytoplasmic + Nuclear + Cytoplasmic Non-SHH/WNT Negative Cytoplasmic - Negative MOLECULAR SUBGROUPS AND IMMUNOREACTIVITY One of the techniques that can be implemented widely across the globe is IHC- based sub classification
- 17. IMMUNOREACTIVITY/ MOLECULAR GROUP WNT SHH Non-SHH/WNT ß-catenin (Nuclear) + - - GAB-1 - + - YAP1 + + - p53 ± Molecular subgroups and immunoreactivity Surrogate IHC Additional for Group 3: c-myc amp (FISH) Additional for WNT: Monosomy Chr 6 (FISH)
- 18. Homer-Wright rosettes composed of neoplastic cells concentrically arranged around fibrillary processes are a common histological feature. Isochromosome17q was confirmed as the most common genetic alteration in medulloblastomas, found in 28% of specimens. Synaptophysin, Neuron enolase, neurofilament protein, tubulin Metastases may have different immunohistology different from the actual primary. PATHOLOGY
- 19. Short time before diagnosis (<3months) Morning headache, vomiting, lethargic Features of raised ICP including papilloedema and diplopia (CN VI) Truncal and appendicular ataxia, nystagmus, bulbar and facial palsy (brainstem), Head tilt (tonsil descent in FM) Macrocrania (infant), Drop mets (Back pain, urinary retention and leg weakness): ~10-35% of MB seeds at the time of dx and Extraneural mets occurs in 5% (sometime promoted by shunt: 10-20%; overestimated ???) CLINICAL PRESENTATION
- 20. Classic features of a medulloblastoma on computed tomographic (CT) scan are increased density on the non-contrast scan, midline location, well-defined margins, and dense, homogeneous enhancement with injection of contrast, surrounding vasogenic edema. Calcification (22%) and cyst formation (59%) The hyperdensity on plain CT scan, seen in medulloblastoma and in some ependymomas, is secondary to the high cellularity of these tumors that have scanty cytoplasm and areas of desmoplasia. WORK UP
- 21. MRI: There is a high degree of variability of MR appearances of medulloblastoma. T1 sequences are usually iso-hypointense to white matter and hyperintense on T2 sequences. Tumor enhancement can be both homogeneous or heterogeneous. Similar to ependymoma, approximately14% of medulloblastomas may show foraminal extension. Banana sign (4th vent drapes around medulloblastoma unlike ependymoma where tumor encroach 4th vent) HCP: 85-90% MRI BRAIN WITH CONTRAST
- 22. T1W-MRI T2W-MRI
- 24. DWI-MRI ADC
- 25. Gd-MRI
- 26. FEATURES MEDULLOBLASTOMA EPENDYMOMAS PILOCYTIC ASTRO HEMANGIOBLASTOMA Origin Roof of 4th V Floor Cerebellar Cerebellar Clinical features Age Acute 5-15 Chronic 3-8 Chronic 5-15 Chronic 40-60 VHL: Young NE-CT Hyperdense (cellularity) Hypo Hypo Hypo Heterogenicity Less More Solid cystic Solid cystic T1W-MRI Hypo Hypo Hypo Hyper (also cyst) T2W-MRI Iso to Hyper Hyper Hyper Hyper, flow void Mural Nodule None None May be present May be present Enhancement Most (E); Non (gr 4) to intense (WNT) Intense Solid enhances Intense Perilesional edema - - - + Calcification Less More None Less Hemorrhage Less More Rare Less Extension into cisternal spaces Less More Nil Less Diffusion restriction Yes No No No MEDULLOBLASTOMA VS EPENDYMOMA
- 27. MR spectroscopy may also be distinctive SHH little or no taurine low creatine Group 3 or 4 Taurine peak high creatine MRS
- 28. MRI SPINE to assess the severity of diseases (Mets) Leptomeningeal seeding on MRI is found in approximately 33% of patients. The spinal canal is the most common location of seeding; however, the supratentorial compartment may also be involved. Nodular or diffuse enhancement along the leptomeninges, nerve roots in the spinal canal, or cranial nerves in the CPA are common findings of CSF seeding. MRI SPINE
- 29. MRI and CSF cytometry may miss 14% of seeding CSF cytometry
- 31. TREATMENT
- 32. 1. Establish histological diagnosis 2. Maximally resect tumor mass 3. Relieve hydrocephalus AIMS OF SURGERY
- 33. MEDULLOBLASTOMA SURGICAL RESECTION HCP TREATED >3 YRS <3 YEARS STANDARD RISK POOR RISK CHEMOTHERAPY FOLLOW UP OR DELAY XRT OR LOCAL FIELD XRT PROTON CSI OR REDUCED DOSE CSI+ CHEMO CSI+ ADJ CHEMO (CCNU, CISPLATIN, VINCRISTINE OR CHEMO ON RESEARCH PROTOCOL FOLLOW RISK STRATIFICATION 1. Age (less than <3 or >3 years); Presence of disseminated disease (M1-4); Extent of surgical resection (<1.5 or >1.5cm residual) and Histological differentiation (5 years PFS among group: 77% vs 35-50%) Better outcome: Girls; WNT:good/ LCA/non SHH/WNT: Poor MEDULLOBLASTOMA FIG: PROPOSED ALGORITHM FOR TREATMENT OF PATIENT WITH MEDULLOBLATOMA XRT: OPTIMAL DOSE 35-40Gy to whole CSI + 10-15 Gy boost to tumor bed (PF) and to any spinal mets, all fractionated over 6-7 weeks Reduce dose by 20-25% or Chemo Chemotherapy improves 5-yr PFS survival (87% vs 33%) Low dose XRT 25 Gy
- 34. Currently risk stratification is based on age (less than 3 years of age), presence of disseminated disease (M1-4, and extent of surgical resection (<1.5 or >1.5cm residual) and histological differentiation along glial, ependymal or neuronal line. (5 yrs PFS among group: 77% vs 53%) In cases in which there is greater than 1.5 cm of residual tumor, a repeat procedure should be considered, if safe and anatomically feasible, to place the patient in the best prognostic category. Medulloblastoma is a radiosensitive tumor and incorporation of radiotherapy has become a standard of care in treatment of children older than 3 years of age. RISK STRATIFICATION PROGNOSTIC FACTORS Low-risk patients. Nuclear accumulation of CTNNB1* CTNNB1* mutations Monosomy stratifies *WNT subgroup markers High-risk patients: MYC/MYCN amplication and isochromosome 17q
- 35. It is generally agreed now that most patients do not require pre-operative shunting. However, 20-35% may need post-operative shunt. Shunt risk of peritoneal dissemination: 10-20%. Pre-operative shunt: Demerit: Tumoral hemorrhage, seeding, upward herniation. If the drain continues to drain at the height of 20cm, hydrocephalus is shown to progress or pseudomeningocele develops. SHUNT OR NOT
- 36. TREATMENT STRATEGY MECHANISM OF ACTION OF CHEMOTHERAPY DRUG MOA SIDE EFFECT CISPLATIN Induces cellular apoptosis by cross-linking DNA Ototoxicity and nephrotoxicity, dys-electrolytemia CYCLOPHOSPHAMIDE Alkylating agent Hemorrhagic cystitis, infertility LOMUSTINE Alkylating agent Myelosuppression, myeloid leukemia VINCRISTINE Microtubule inhibitor that prevents cell division by binding to the tubulin component of microtubules and leading to metaphase arrest Peripheral neuropathy. Muscle weakness, SEVERE CONSTIPATION
- 37. Radiation therapy (XRT) should begin ~30 days following definitive surgery. Historically, the entirety of the cerebellum was radiated. Therapy is delivered in daily fractions of 1.8 Gy to a final dose of 54 Gy - 59.4 Gy. Craniospinal irradiation (CSI) is delivered to the entire brain and spine and given concurrently with primary site radiation for the first 13 days of therapy, to a total dose of 23.4 Gy (1.8x 13days) RADIOTHERAPY Posterior fossa ®: 1.8 Gy for 1 months (54-59.4 Gy) CSI ®: 1.8 Gy for 13 days (23.4 Gy) MEDULLOBLASTOMA
- 38. The current standard of care for average risk medulloblastoma among >3 yrs child is gross total resection, postoperative craniospinal radiation of 23.4 Gy with a tumor bed irradiation t of 54 Gy, followed by 12 months of chemotherapy. Cyclophosphamide, vincristine, cisplatin and peripheral stem cell rescue. (5 years EFS ~70%) Child <3 years: chemotherapy has been used to delay radiation therapy until nervous system matures or reduced (20-25% of total) dose of XRT. Administration of focal radiation to tumor bed is insufficient to control medulloblastoma, even if there is no evidence of disseminated disease at diagnosis. Consequently, irradiation of entire neuraxis is critical in the treatment of medulloblastoma. CURRENT STANDARD OF CARE
- 39. Cognitive decline, endocrine insufficiency, hearing loss, growth retardation, vascular complications, leukoencephalopathy and secondary malignancies. SIDE EFFECTS OF RADIATION
- 40. Proton therapy: Bragg peak: capacity to deliver targeted radiation while sparing normal structure. Target avoiding spinal growth plate, auditory canal, pituitary fossa. NOVEL IRRADIATION PROMISE
- 41. MRI within 48 hours to minimize detection of non-tumoral post-operative changes Postoperative surveillance imaging of the brain and spine in patients with medulloblastoma is routinely employed at many institutions with 3–6 month intervals during the first 5 years following initial diagnosis in the hope of detecting recurrent disease earlier. . POST OP IMAGING
- 42. Post op neurological morbidity: 25-57% Cerebral mutism (25%); Dysarthria persist after mutism recover. Recurrence: Collin’s law to define period of recurrence (age at diagnosis + 9 months; Autologous stem cell rescue to deliver chemotherapy at dose that may provide better response was tried limited by hematologic toxicity. OUTCOME
- 43. 5 years survival: M0: 70% M1: 57% M ≥2: 40% Prognosis is most strongly influenced by molecular subtype WNT: very good SHH: infants good, others intermediate group 3: poor group 4: intermediate Outcome is good among girls Recurrence occurs in duration of 4-20 months. Survival after recurrence: 5months (poor) PROGNOSIS
- 44. Expression of the c-erbB-2 (HER2/neu) oncogene is useful in the staging of medulloblastomas. Increased c-erbB-2 expression reflects an increase in the proliferative activity of a tumor (widely used in breast cancer staging). No CSF metastases, complete surgical resection and negative c-erbB-2 expression: 5-year-survival 100%. No CSF metastases, complete surgical resection and positive c-erbB-2 expression: 5-year-survival 54%. CSF metastases and/or incomplete surgical resection: 5-year-survival 20%. c-erbB-2 (HER2/neu) oncogene expression
- 45. Protein phosphatase inhibitor Norcantharidin for WNT: + nuclear B- catenin. Smoothened (SMO) inhibitors: Vismodegib and Sonidegib targets Shh pathway Suppress MYC-related pathway activity. FUTURE
- 46. GOOD 1. WNT 2. B Catenin 3. Classic, Desmoplastic CONFOUNDERS OF OUTCOME BAD 1. GAB1, YAB1 2. TP53 3. Large/Anaplastic 4. MYC amplification
- 47. Thank you NATIONAL INSTITUTE OF NEUROLOGICAL AND ALLIED SCIENCES, BANSBARI, KATHMANDU MEDULLOBLASTOMA UPENDRA DEVKOTA MEMORIAL NATIONAL INSTITUTE OF NEUROLOGICALAND ALLIED SCIENCES, BANSBARI, KATHMANDU