
Recommended
More Related Content
What's hot
What's hot (20)
Similar to PLACENTAL ABRUPTION: CAUSES, SIGNS & TREATMENT
Similar to PLACENTAL ABRUPTION: CAUSES, SIGNS & TREATMENT (20)
More from Babitha Mathew
Recently uploaded
Recently uploaded (20)
PLACENTAL ABRUPTION: CAUSES, SIGNS & TREATMENT
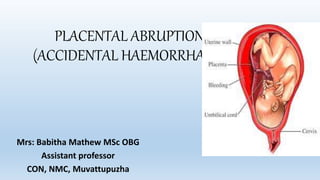
- 1. PLACENTAL ABRUPTION (ACCIDENTAL HAEMORRHAGE) Mrs: Babitha Mathew MSc OBG Assistant professor CON, NMC, Muvattupuzha
- 2. PLACENTAL ABRUPTION •It is one form of antepartum hemorrhage where the bleeding occurs due to premature separation of normally situated placenta.
- 3. TYPES OF ABRUPTION depending upon the extent and region of separation. • A complete abruption occurs when the entire placenta separates. • A partial abruption exists when part of the placenta separates from the uterine wall. •A marginal abruption occurs when the separation is limited to the edge of the placenta
- 4. VARIETIES •(1) Revealed : Following separation of the placenta, the blood insinuates downwards between the membranes and the decidua. Ultimately, the blood comes out of the cervical canal to be visible externally. This is the commonest type.
- 5. • (2) Concealed : The blood collects behind the separated placenta or collected in between the membranes and decidua. The collected blood is prevented from coming out of the cervix by the presenting part which presses on the lower segment.
- 6. (3) Mixed : •In this type, some part of the blood collects inside (concealed) and a part is expelled out (revealed). •Usually one variety predominates over the other. This is quite common.
- 7. RISK FACTORS 1)The prevalence is more with •(a) high birth order pregnancies with gravida 5 and above — three times more common than in first birth •(b) advancing age of the mother •(c) poor socio-economic condition •(d) malnutrition •(e) smoking (vaso-spasm).
- 8. 2)Hypertension in pregnancy • Pre-eclampsia, gestational hypertension and essential hypertension, all are associated with placental abruption. •The mechanism of the placental separation in pre- eclampsia is : Spasm of the vessels in the utero placental bed (decidual spiral artery) → anoxic endothelial damage → rupture of vessels or extravasation of blood in the decidua basalis (retroplacental hematoma).
- 9. 3)Trauma: Traumatic separation of the placenta usually leads to its marginal separation with escape of blood outside. The trauma may be due to: (i) Attempted external cephalic version specially under anaesthesia using great force (ii) Road traffic accidents or blow on the abdomen (iii) Needle puncture at amniocentesis.
- 10. 4) Sudden uterine decompression: Sudden decompression of the uterus leads to diminished surface area of the uterus adjacent to the placental attachment and results in separation of the placenta. This may occur following— (a)delivery of the first baby of twins (b) sudden escape of liquor amnii in hydramnios and (c) premature rupture of membranes.
- 11. 5) Short cord, either relative or absolute, can bring about placental separation during labor by mechanical pull. 6) Supine hypotension syndrome: In this condition which occurs in pregnancy there is passive engorgement of the uterine and placental vessels resulting in rupture and extravasation of the blood. 7) Placental anomaly: Circumvallate placenta 8) Sick placenta: Poor placentation, 9) Folic acid deficiency
- 12. 10) Uterine factor: Placenta implanted over a septum (Septate Uterus) or a submucous fibroid. 11) Torsion of the uterus leads to increased venous pressure and rupture of the veins with separation of the placenta. 12)Cocaine abuse is associated with increased risk of transient hypertension, vasospasm and placental abruption. 13)Thrombophilias inherited or acquired have been associated with increased risk of placental infarcts or abruption. 14)Prior abruption: Risk of recurrence for a woman with previous abruption varies between 5 to 17%.
- 14. CLINICAL CLASSIFICATION: Depending upon the degree of placental abruption and its clinical effects Grade—0: • Clinical features may be absent. • The diagnosis is made after inspection of placenta following delivery. Grade—1 (40%): • (i) Vaginal bleeding is slight • (ii)Uterus:irritable, tenderness may be minimal or absent • (iii) Maternal BP and fibrinogen levels unaffected • (iv) FHS is good. (i) Vaginal bleeding mild to moderate (ii) Uterine tenderness is always present (iii) Maternal pulse ↑, BP is maintained (iv) Fibrinogen level may be decreased (v) Shock is absent (vi) Fetal distress or even fetal death occurs. Grade—2 (45%): (i) Bleeding is moderate to severe or may be concealed (ii) Uterine tenderness is marked (iii) Shock is pronounced (iv) Fetal death is the rule (v) Associated coagulation defect or anuria may complicate. Grade—3 (15%):
- 15. CLINICAL MANIFESTATION Clinical manifestation mild moderate severe Per vaginal bleeding No overt per vaginal bleeding Moderate vagnal bleeding Massive vaginal bleeding Rigid abdomen Present Present Present Blood pressure Decreased Decreased Decreased Pulse Tachycardia Tachycardia Tachycardia Accute abdominal pain Present Present Present Shock Not May/may not Present Uteroplacental insufficiancy present present Markedly present
- 17. Revealed Mixed (Concealed features predominate)
- 18. MANAGEMENT OF ABRUPTIO PLACENTAE •Prevention: The prevention aims at— •(1) elimination of the known factors likely to produce placental separation •(2) correction of anemia during antenatal period so that the patient can withstand blood loss and •(3) prompt detection and institution of the therapy to minimise the grave complications namely shock, blood coagulation disorders and renal failure.
- 19. Prevention • • Early detection and effective therapy of pre-eclampsia and other hypertensive disorders of pregnancy. • • Needle puncture during amniocentesis should be under ultrasound guidance. • • Avoidance of trauma—specially forceful external cephalic version under anesthesia. • To avoid sudden decompression of the uterus— in acute or chronic hydramnios, amniocentesis is preferable to artificial rupture of the membranes. • • To avoid supine hypotension the patient is advised to lie in the left lateral position in the later months of pregnancy. • • Routine administration of folic acid from the early pregnancy — of doubtful value.
- 20. AT HOME: • The patient is to be treated as outlined in placenta previa and arrangement should be made to shift • the patient to an equipped maternity unit as early as possible. • IN THE HOSPITAL: • Assessment of the case is to be done as regards: (a) amount of blood loss (b) maturity of the fetus and (c) whether the patient is in labor or not (usually labor starts) (d) presence of any complication and (e) type and grade of placental abruption
- 21. • Management options (a) Immediate delivery (b) Management of complications if there is any (c) Expectant management (rare). •Definitive treatment (immediate delivery): • The patient is in labor: Most patients are in labor following a term pregnancy: The labor is accelerated by low rupture of the membranes. Rupture of the membranes with escape of liquor amnii accelerates labor and it increases the uterine tone also. • Oxytocin drip may be started to accelerate labor when needed. • Vaginal delivery is favored in cases with: (i) Limited placental abruption (ii) FHR tracing reassuring (iii) Facilities for continuous (electronic) fetal monitoring is available (iv) Prospect of vaginal delivery is soon or (v) Placental abruption with a dead fetus.
- 22. The patient is not in labor: (i) Bleeding continues (ii) > Grade I abruption Delivery either by (A) Induction of labor or (B) Cesarean section. Indications are : (a) Severe abruption with live fetus (b) Amniotomy could not be done (unfavorable cervix) (c) Prospect of immediate vaginal delivery despite amniotomy is remote (d) Amniotomy failed to control bleeding (e) Amniotomy failed to arrest the process of abruption (rising fundal height) (f) Appearance of adverse features (fetal distress, falling fibrinogen level, oliguria).
- 23. DIGNOSIS • Clinical grounds of painful vaginal bleeding in association with uterine tenderness & hyperactivity • USG demonstrate retro placental clots & to exclude placenta preavia • Abruption may occur in the absence of US findings. • In some cases the diagnosis may be only made by inspection of placenta after 3rd stage of labour MANAGEMENT • Careful maternal haemodynamic monitoring • Fetal monitoring • fluid administration • Serial evaluation of the haematocrit & coagulation profile • Expectant management (preterm patients with less severe abruptions an minimal bleeding) • Delivery of the fetus • Vaginal (ARM & oxytocin) fetal death mild to mod abruption with no fetal distress or CI • Cesarean fetal distress
- 24. COMPLICATIONs MATERNAL • 1. Maternal mortality 1% • 2. Recurrence of APH in 10% & ↑to 25% after 2nd episodes • 3. Hypovolemic shock -concealed • 4. Acute renal failure- ATN • 5. DIC- Abruption is the most common cause of coagulopathy in pregnancy low plt and fibrinogen, prolonged PT/a PTT • 6. PPH -coagulation failure /Couvelaire uterus-Rarely, blood penetrates the uteru to such an extent that the serosa becomes blue or purple in colour. • 7. Feto-maternal haemorrhage lead to severe Rh sensitization in Rh • negative mother • - A Kleihauer-Betke or similar test is essential FETAL • 1. Perinatal mortality: • 4.5 % - 60% depending on • neonatal facilities & closely • related to the gestational age & associated complication like HTN & growth restriction • 2. IUGR due to presence of maternal hypertension & pre eclampsia • 3. Neonatal anemia
- 25. • •
- 26. Clinical features PLACENTA PREVIA ABRUPTIO PLACENTAE • nature of bleeding • character of blood • general condition and anemia • features of preeclampsia •Bleeding (duration) • painless -causeless and recurrent, always revealed •bright red • proportionate to visible blood loss ------- Often ceases within 1-2 hrs • painful, cont. revealed/concealed •dark coloured out of proportion in concealed or mixed present in one third cases Continuous Abdominal examination • height of the uterus • feel of uterus • malpresentation • FHS •DIC •Associated history • proportionate • soft and relaxed • common, head is high floating •Present •Normal •rare • disproportionate (concealed) • tense, tender and rigid --------------- • absent in concealed. TC then BC, Loss of variability, Decelerations, IUFD Severe •Trauma, hypertension Multiple gestation Polyhydramnios Placentography US placenta in lower segment Placentography US placenta in lower segment Placenta in upper segment Vaginal examination Placenta felt on the lower segment Placenta not felt