
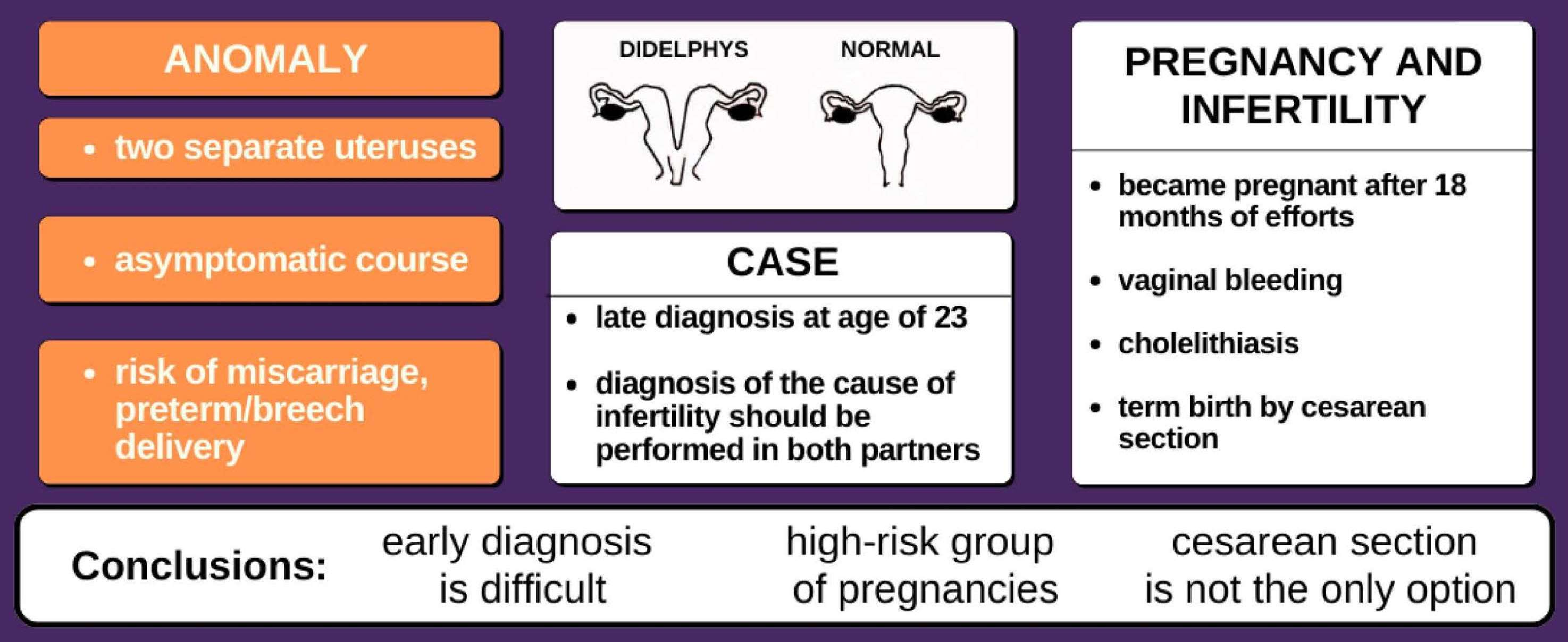
The Impact of Uterus Didelphys on Fertility and Pregnancy

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Case Report
2.1. Gynecological History of the Patient
2.2. Infertility and Partner
2.3. Pregnancy
2.4. Labor
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grimbizis, G.F.; Camus, M.; Tarlatzis, B.C.; Bontis, J.N.; Devroey, P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum. Reprod. Update 2001, 7, 161–174. [Google Scholar] [CrossRef]
- Slavchev, S.; Kostov, S.; Yordanov, A. Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases. Medicina (B Aires) 2020, 56, 198. [Google Scholar] [CrossRef]
- Moore, K.L.; Persaud, V. Before We Are Born–Essentials of Human Embryology and Birth Defects; Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Rezai, S.; Bisram, P.; Alcantara, I.L.; Upadhyay, R.; Lara, C.; Elmadjian, M. Didelphys Uterus: A Case Report and Review of the Literature. Case Rep. Obstet. 2015, 2015, 865821. [Google Scholar] [CrossRef] [PubMed]
- Acién, P.; Acién, M. The presentation and management of complex female genital malformations. Hum. Reprod. Update 2016, 22, 48–69. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.M.; Kane, S.C.; Haines, T.P.; Sheehan, P.M. Cervical length surveillance for predicting spontaneous preterm birth in women with uterine anomalies: A cohort study. Acta Obstet. Et Gynecol. Scand. 2020, 99, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Buttram, V.C.; Gomel, V.; Siegler, A.; DeCherney, A.; Gibbons, W.; March, C. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar] [CrossRef]
- Pfeifer, S.M.; Attaran, M.; Goldstein, J.; Lindheim, S.R.; Petrozza, J.C.; Rackow, B.W.; Siegelman, E.; Troiano, R.; Winter, T.; Zuckerman, A.; et al. ASRM müllerian anomalies classification 2021. Fertil. Steril. 2021, 116, 1238–1252. [Google Scholar] [CrossRef]
- Fox, N.S.; Roman, A.S.; Stern, E.M.; Gerber, R.S.; Saltzman, D.H.; Rebarber, A. Type of congenital uterine anomaly and adverse pregnancy outcomes. J. Matern. Fetal Neonatal Med. 2014, 27, 949–953. [Google Scholar] [CrossRef]
- Chan, Y.Y.; Jayaprakasan, K.; Tan, A.; Thornton, J.G.; Coomarasamy, A.; Raine-Fenning, N.J. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obstet. Gynecol. 2021, 38, 2011. [Google Scholar] [CrossRef]
- Mohamed, M.A.; AbdelRahman, M.Y. Frequency and types of uterine anomalies during caesarean section. J. Obstet. Gynaecol. 2019, 39, 147–150. [Google Scholar] [CrossRef]
- Garcia-Flores, V.; Romero, R.; Furcron, A.-E.; Levenson, D.; Galaz, J.; Zou, C.; Hassan, S.S.; Hsu, C.-D.; Olson, D.; Metz, G.A.S.; et al. Prenatal Maternal Stress Causes Preterm Birth and Affects Neonatal Adaptive Immunity in Mice. Front. Immunol. 2020, 11, 254. [Google Scholar] [CrossRef]
- Damiani, G.R.; Gaetani, M.; Landi, S.; Lacerenza, L.; Barnaba, M.; Spellecchia, D.; Pellegrino, A. Uterine rupture in a nulliparous woman with septate uterus of the second trimester pregnancy and review in literature. Int. J. Surg. Case Rep. 2013, 4, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, X.; Sha, S.; Yao, L.; Zhu, X.; Shao, Y. Delayed presentation of uterine rupture in a didelphys uterus misdiagnosed as appendicitis: A case report and review of the literature. Arch. Gynecol. Obstet. 2017, 296, 1015–1016. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, C.; Sun, M.; Li, H.; Cao, Y.; Wei, Z. Spontaneous unscarred uterine rupture in a twin pregnancy complicated by adenomyosis A case report. Medicine 2021, 100, e24048. [Google Scholar] [CrossRef] [PubMed]
- Loverro, M.T.; Damiani, G.R.; Di Naro, E.; Schonauer, L.M.; Laforgia, N.; Loverro, M.; Capursi, T.; Muzzupapa, G.; Resta, L. Analysis of relation between placental lesions and perinatal outcome according to Amsterdam criteria: A comparative study. Acta Biomedica 2020, 91, e2020061. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.-A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and definitions of placental lesions Amsterdam placental workshop group consensus statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef]
- Khander, A.; Stern, E.; Gerber, R.S.; Fox, N.S. The association between obstetrical history and preterm birth in women with uterine anomalies. J. Matern. -Fetal Neonatal Med. 2018, 31, 2550–2554. [Google Scholar] [CrossRef]
- Jorgensen, C.; Lusiak, M. Didelphys Uterus in Pregnancy, an Uncommon Mullerian Duct Anomaly: A Case Report. Clin. Pract. Cases Emerg. Med. 2021, 5, 447–449. [Google Scholar] [CrossRef]
- Khrait, Z. Embryo transfer can be performed in either uterine horn. Two successive pregnancies in a patient with uterus didelphys: A case report. J. Med. Case Rep. 2021, 15, 1–5. [Google Scholar] [CrossRef]
- King, A.L.; Pixton, S.; Lanzarone, V. Uterine didelphys with dicavitary twin gestation: A case report. Case Rep. Women’s Health 2020, 27, e00199. [Google Scholar] [CrossRef]
- Post, R.J.; Templeman, C.L.; Benoit, R.M. Twin gestation in a uterus didelphys with only one functional cervix: A case report. Case Rep. Women’s Health 2019, 22, e00118. [Google Scholar] [CrossRef] [PubMed]
- Goulios, C.; McCuaig, R.; Hobson, L.; White, S. Management of a twin pregnancy in a didelphys uterus: One fetus in each uterine cavity. BMJ Case Rep. 2020, 13, e235256. [Google Scholar] [CrossRef] [PubMed]
- al Yaqoubi, H.N.; Fatema, N. Successful Vaginal Delivery of Naturally Conceived Dicavitary Twin in Didelphys Uterus: A Rare Reported Case. Case Rep. Obstet. Gynecol. 2017, 2017, 1–4. [Google Scholar] [CrossRef]
- Mohamad, K.R.; Saheb, W.; Jarjour, I.; El-Tal, R.; Malas, A.; Meita, Z.; Badr, D.A. Delayed-interval-delivery of twins in didelphys uterus complicated with chorioamnionitis: A case report and a brief review of literature. J. Matern. Fetal Neonatal Med. 2020, 35, 3318–3322. [Google Scholar] [CrossRef]
- Ross, C.; El-Hassan, H.; Lakasing, L. Uterus didelphys: Two pregnancies, two term breech caesarean deliveries. BMJ Case Rep. 2018, 2018, bcr-2017. [Google Scholar] [CrossRef]
- Jan, H.; Bizrah, M.; Hamid, R. A case of spontaneous conceived twins in uterus didelphys, with induction and delayed delivery between twins. J. Obstet. Gynaecol. 2013, 33, 525–526. [Google Scholar] [CrossRef] [PubMed]
- Altwerger, G.; Pritchard, A.M.; Black, J.D.; Sfakianaki, A.K. Uterine didelphys and vaginal birth after cesarean delivery. Obstet. Gynecol. 2015, 125, 157–159. [Google Scholar] [CrossRef]
- Ng’Ang’A, N.; Ratzersdorfer, J.; Abdelhak, Y. Vaginal birth after two previous caesarean deliveries in a patient with uterus didelphys and an interuterine septal defect. BMJ Case Rep. 2017, 2017, bcr-2016. [Google Scholar] [CrossRef]
- Ng, K.S.; Ng, B.K.; Lim, P.S.; Shafiee, M.N.; Karim, A.K.A.; Omar, M.H. Use of hydroxyprogesterone caproate to prevent preterm labour in uterine didelphys: A case report. Horm. Mol. Biol. Clin. Investig. 2016, 27, 89–91. [Google Scholar] [CrossRef]
- Cheng, C.; Tang, W.; Zhang, L.; Luo, M.; Huang, M.; Wu, X.; Wan, G. Unruptured pregnancy in a noncommunicating rudimentary horn at 37 weeks with a live fetus: A case report. J. Biomed. Res. 2015, 29, 83–86. [Google Scholar] [CrossRef]
- Kabadi, Y.M.; Ayyanar, A. A ‘cluster’ of ten uterine anomalies observed in a single center over a short period of 4 weeks: A case series. J. Med. Case Rep. 2022, 16, 130. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.J.; Tseng, J.Y.; Chen, C.Y.; Li, H.Y. Delivery of double singleton pregnancies in a woman with a double uterus, double cervix, and complete septate vagina. J. Chin. Med. Assoc. 2015, 78, 746–748. [Google Scholar] [CrossRef]
- Adams, T.; Sharma, S.; Kinzler, W.L.; Vintzileos, A.M. Transvaginal sonographic monitoring of cervical length in uterus didelphys. J. Ultrasound Med. 2014, 33, 917–918. [Google Scholar] [CrossRef] [PubMed]
- Cappello, S.; Piccolo, E.; Cucinelli, F.; Casadei, L.; Piccione, E.; Salerno, M.G. Successful preterm pregnancy in a rare variation of Herlyn-Werner-Wunderlich syndrome: A case report. BMC Pregnancy Childbirth 2018, 18, 498. [Google Scholar] [CrossRef] [PubMed]
- Živković, K.; Prka, M.; Živković, N.; Bucko, A.; Habek, D. Unusual case of OHVIRA syndrome with a single uterus, unrecognized before labor and followed by an intrapartal rupture of obstructed hemivagina. Arch. Gynecol. Obstet. 2014, 498, 290. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Chai, W.; Cui, M.; Wen, Y.; Cui, L.; Gong, F. A case report on Herlyn–Werner–Wunderlich syndrome with spontaneous abortion. Medicine 2018, 97, e12004. [Google Scholar] [CrossRef] [PubMed]
- Wielgos, M.; Bomba-Opoń, D.; Breborowicz, G.H.; Czajkowski, K.; Debski, R.; Leszczynska-Gorzelak, B.; Oszukowski, P.; Radowicki, S.; Zimmer, M. Recommendations of the Polish Society of Gynecologists and Obstetricians regarding caesarean sections. Ginekol. Pol. 2018, 89, 644–657. [Google Scholar] [CrossRef]
- Gray, C.J.; Shanahan, M.M. Breech Presentation; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Heinonen, P.K. Uterus didelphys: A report of 26 cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 1984, 17, 345–350. [Google Scholar] [CrossRef]
- Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation: Green-top Guideline No. 20b. BJOG: Int. J. Obstet. Gynaecol. 2017, 124, 20. [Google Scholar] [CrossRef]
- Mirzai, S.; Wolf, S.B.; Mili, S.; Rifai, A.O. Successful external cephalic version in a patient with uterus didelphys and fetal malpresentation. BMJ Case Rep. 2019, 12, e230965. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Age of Dia-Gnosis | Age of Pre-Gna-Ncy | Presence of a Vaginal Septum | Fetus in the Right/Left Uterus | Position of the Fetus | Natural Childbirth/ Cesarean Section | Indications for Cesarean Section | References |
|---|---|---|---|---|---|---|---|
| 23 | 26 | present | left | longitudinal cephalic | cesarean section | the strong fear of the patient for the baby and presence of septum in the vagina | the case described in this article |
| 35 | 35 | present | right | breech presentation | cesarean section | breech presentation | [19] |
| 28 | 29 | present | left | anterior presentation | natural childbirth | N/A | [4] |
| 20 | 21 | present | left | ND | cesarean section | ND | [2] |
| 25 | 25 | absent | left | frontal occipitoparietal position | cesarean section | no progress in labor | [2] |
| 27 | 27 | present | right | frontal occipitoparietal position | natural childbirth | N/A | [2] |
| 27 | 35 | absent | right | ND | cesarean section | ND | [20] |
| 27 | 27 | absent (removed in the past) | twin pregnancy | ND | 1—natural childbirth (right uterus); 2—cesarean section (left uterus) | chorio- amnionitis | [21] |
| ND | 35 | ND | twin pregnancy | ND | cesarean section | it was uncertain whether the left twin would be able to be delivered vaginally | [22] |
| 29 | 35 | absent (removed in the past) | twin pregnancy | breech presentation | cesarean section | breech presentation | [23] |
| ND | 30 | present | twin pregnancy | ND | natural childbirth | N/A | [24] |
| 36 | 36 | ND | twin pregnancy | ND | cesarean section | chorio-amnionitis | [25] |
| 26 | 34 | ND | left | breech presentation | cesarean section | breech presentation | [26] |
| ND | 26 | present | twin pregnancy | ND | natural childbirth (delayed delivery between twins) | ND | [27] |
| ND | 30 | present | right | occiput posterior position | natural childbirth | N/A | [28] |
| 18 | 23 | absent (removed in the past) | left | anterior presentation | natural childbirth | N/A | [29] |
| ND | 36 | ND | right | cephalic presentation | cesarean section | status after two cesarean sections | [30] |
| 25 | 25 | ND | right | breech presentation | cesarean section | primigravida, breech presentation with suspected intra-hepatic cholestasis of pregnancy and uterine malformation | [31] |
| 20 | 20 | present | ND | ND | cesarean section | risk of rupture of a scar from a previous pregnancy | [32] |
| 19 | 19 | present | ND | N/A | case with 9 weeks of gestation underwent manual vacuum aspiration (MVA) | N/A | [32] |
| 37 | 37 | present | twin pregnancy | cephalic presentation | cesarean section | the fetus in the uterus with the rarely dilated vagina was expected to present a difficult delivery, an unpredictable labor course might occur arising from the competition of two simultaneously laboring uteruses | [33] |
| ND | 34 | absent | twin pregnancy | ND | natural childbirth | N/A | [34] |
| ND | 28 | absent (removed in the past) | ND | breech presentation | cesarean section | breech presentation | [35] |
| 28 | 30 | absent | ND | cephalic position | natural childbirth | N/A | [36] |
| 22 | 22 | present | left | ND | spontaneous abortion | ND | [37] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćwiertnia, A.; Borzyszkowska, D.; Golara, A.; Tuczyńska, N.; Kozłowski, M.; Kwiatkowski, S.; Cymbaluk-Płoska, A. The Impact of Uterus Didelphys on Fertility and Pregnancy. Int. J. Environ. Res. Public Health 2022, 19, 10571. https://doi.org/10.3390/ijerph191710571
Ćwiertnia A, Borzyszkowska D, Golara A, Tuczyńska N, Kozłowski M, Kwiatkowski S, Cymbaluk-Płoska A. The Impact of Uterus Didelphys on Fertility and Pregnancy. International Journal of Environmental Research and Public Health. 2022; 19(17):10571. https://doi.org/10.3390/ijerph191710571
Chicago/Turabian StyleĆwiertnia, Adrianna, Dominika Borzyszkowska, Anna Golara, Natalia Tuczyńska, Mateusz Kozłowski, Sebastian Kwiatkowski, and Aneta Cymbaluk-Płoska. 2022. "The Impact of Uterus Didelphys on Fertility and Pregnancy" International Journal of Environmental Research and Public Health 19, no. 17: 10571. https://doi.org/10.3390/ijerph191710571