Homeopathic Treatment of Addison’s Disease
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines selected after a full individualizing examination and case-analysis.
which includes
- The medical history of the patient,
- Physical and mental constitution,
- Family history,
- Presenting symptoms,
- Underlying pathology,
- Possible causative factors etc.
A miasmatic tendency (predisposition/susceptibility) also often taken into account for the treatment of chronic conditions.
What Homoeopathic doctors do?
A homeopathy doctor tries to treat more than just the presenting symptoms. The focus is usually on what caused the disease condition? Why ‘this patient’ is sick ‘this way’?.
The disease diagnosis is important but in homeopathy, the cause of disease not just probed to the level of bacteria and viruses. Other factors like mental, emotional and physical stress that could predispose a person to illness also looked for. No a days, even modern medicine also considers a large number of diseases as psychosomatic. The correct homeopathy remedy tries to correct this disease predisposition.
The focus is not on curing the disease but to cure the person who is sick, to restore the health. If a disease pathology not very advanced, homeopathy remedies do give a hope for cure but even in incurable cases, the quality of life can greatly improved with homeopathic medicines.
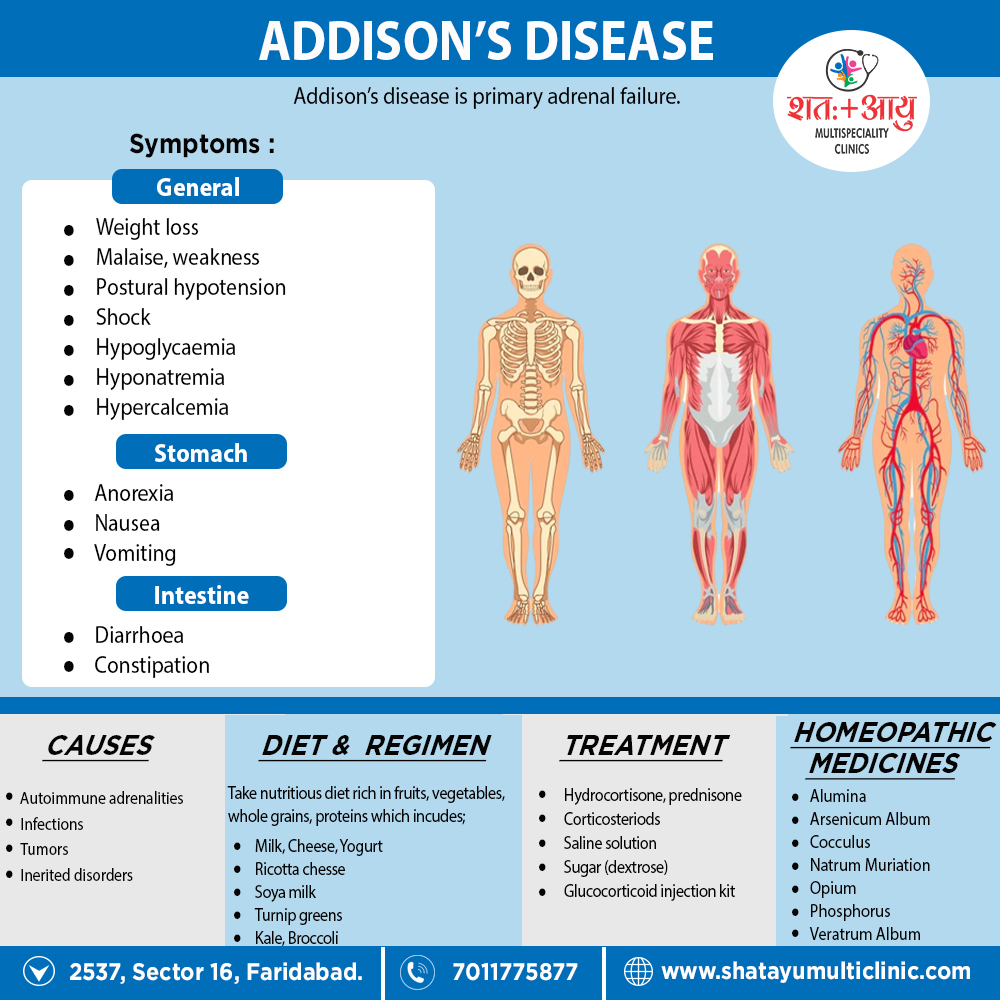
Homeopathic medicines for Addison’s Disease:
The homeopathic remedies (medicines) given below indicate the therapeutic affinity but this is not a complete and definite guide to the homeopathy treatment of this condition. The symptoms listed against each homeopathic remedy may not be directly related to this disease because in homeopathy general symptoms and constitutional indications also taken into account for selecting a remedy.
Alumina:
- Dryness of mucous membranes.
- Eructation in spare, dry, but thin.
- Old people or prematurely aged. No desire to eat. Can swallow but small morsels at a time.
- Especially, indicated when confused as to personal identity. Low-spirited. Constipation. Menses scanty, pale.
- Worse – cold air, after eating, standing. On the other hand, Better – warmth, fasting, resting in bed.
Arsenic album:
- Gradual loss of weight from impaired nutrition.
- Great anguish also restlessness.
- General sensibility increased.
- Cannot bear either the sight or smell of food.
- Nausea, retching, vomiting after eating or drinking. Particularly, in anxiety in pit of stomach.
Cocculus:
- For travel nausea and sickness.
- Fever is gone but the patient does not rally, there is much nervous trembling, numbness, twitching of muscles and great weakness.
- Violent attacks of gastralgia, due to violent cramp of the stomach. Griping, pinching, constrictive pain.
- From grief ,anxiety, and from prolonged loss of sleep. Also in Headache, vertigo, nausea.
- The woman is emaciated, and grows more and more sickly and chlorotic. [5]
Natrum Muriaticum:
- Great weakness and weariness.
- Especially indicated when oversensitive to all sorts of influences.
- Depressed particularly in chronic diseases. Hungry, yet loose flesh.
- Unquenchable thirst.
- Sweats while eating. Wants to be alone to cry.
- Tears with laughter.
- Menses either irregular or suppressed. Additionally, heart fluttering or palpitation
Opium:
- With either coma or complete inactivity.
- Extremities and face are either bluish or a livid colour.
- Loud breathing, convulsions also trembling.
Phosphorus:
- Firstly, A picture of phosphorus for Addison’s Disease is, destructive metabolism.
- Secondly, thin, transparent skin weakened by loss of animal-fluids, with great nervous debility and emaciation.
- Then, Great lowness of spirits. Easily vexed. Fearful.
- Throws up ingest by mouthfuls.
- The food scarcely swallowed, comes up again. Additionally, pain in stomach relieved by cold food.
- Long, narrow, hard stools difficult to expel. Also, Amenorrhoea.
- At last, heart violent palpitations with anxiety.[4]
Veratrum album:
- Cold sweat on forehead also body.
- Marked by violence and destructiveness; wants to destroy, to tear something; tears the clothes from the body. In Addition, always wants to be busy, to carry on his daily work.
- Vomiting forcible and excessive.
- After that, nausea with weakness; is obliged to lie down
- intense cramps in the stomach; similarly, cramps in the muscles of the abdomen like colic. [5]