- Etiology: abnormal cortical organization secondary to ischemic laminar necrosis of 5th cortical layer after 20 weeks gestation, may be caused by in-utero cytomegalovirus, in-utero ischemia, or chromosomal mutation
- Imaging: usually multiple small gyri, too few sulci, focal or diffuse, unilateral or bilateral, in and around Sylvian fissure, anomalous venous drainage in 50%, sometimes indistinguishable from pachygyria
- DDX: gyri of polymicrogyria cannot be named by textbook while gyri of lissencephaly can be named by textbook though simplified
- Complications:
- Treatment:
- Clinical:
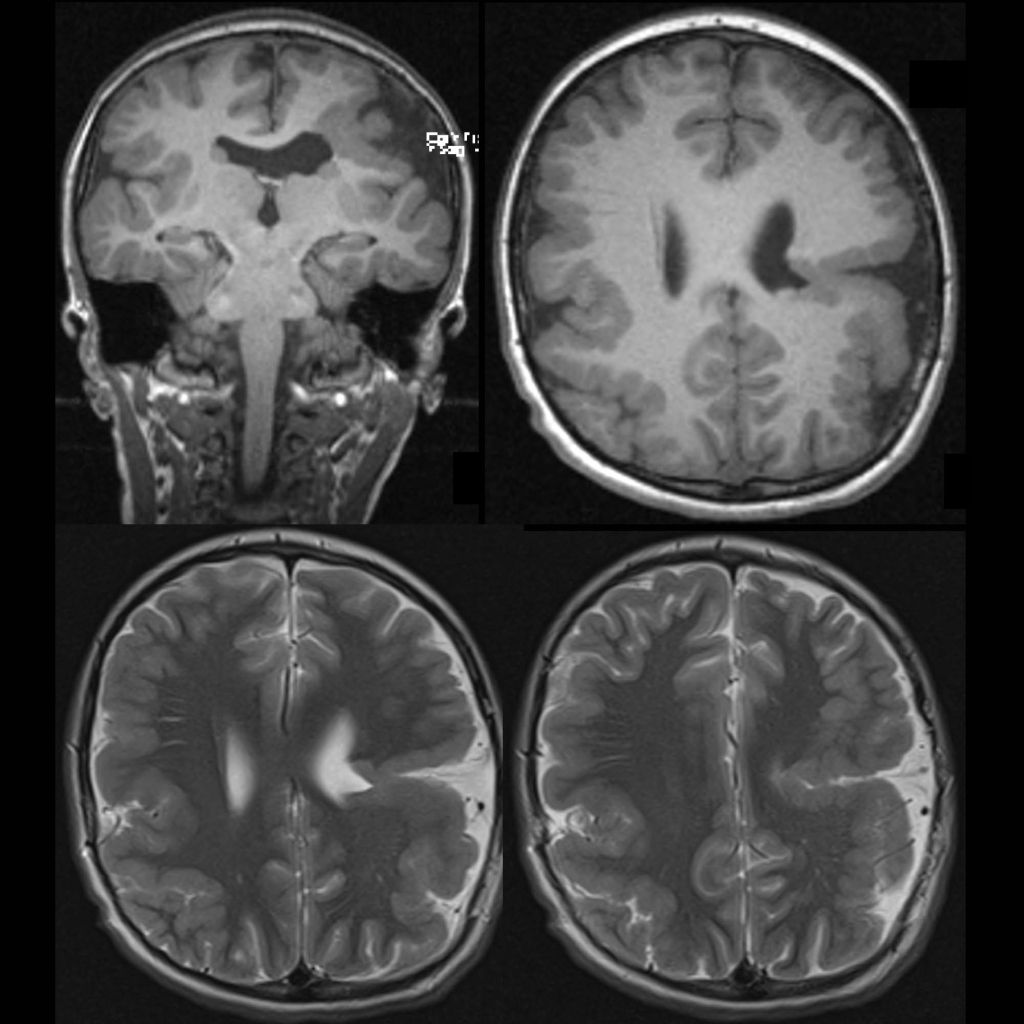
Radiology Cases of Polymicrogyria