- Etiology: can be primary or secondary, anterior middle cranial fossa most common, left > right, large size range
- Imaging: circumscribed CSF signal collection, most don’t change substantially over time especially in children > 4 years old
- DDX:
- Complications: spontaneous rupture of cysts causing subdural hygroma is uncommmon – contact sports may be restricted with large cysts, intracystic hemorrhage after trauma rare
- Treatment: indicated if causing clear and specific neurologic symptoms, mass effect alone not indication for surgery
- Clinical: very common – 2% of scans, usually asymptomatic and incidental
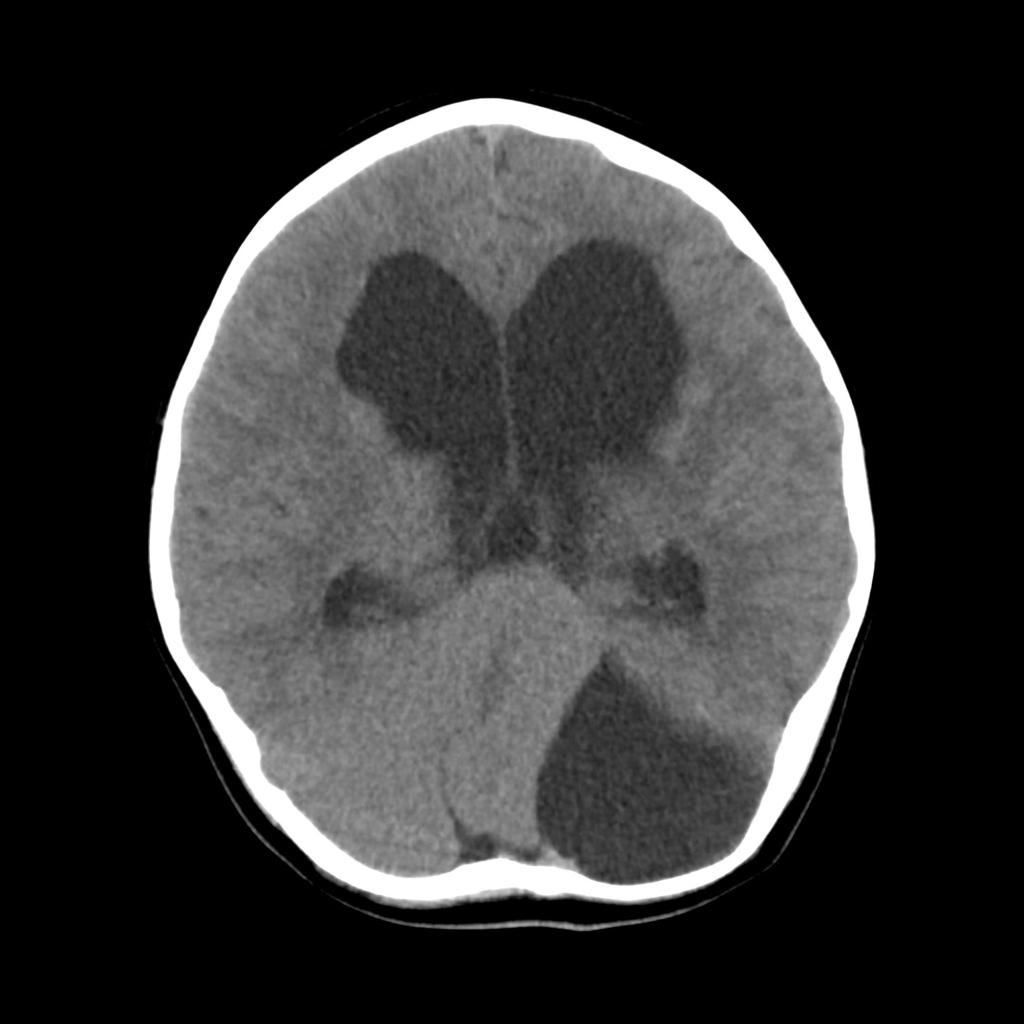
Radiology Cases of Arachnoid Cyst

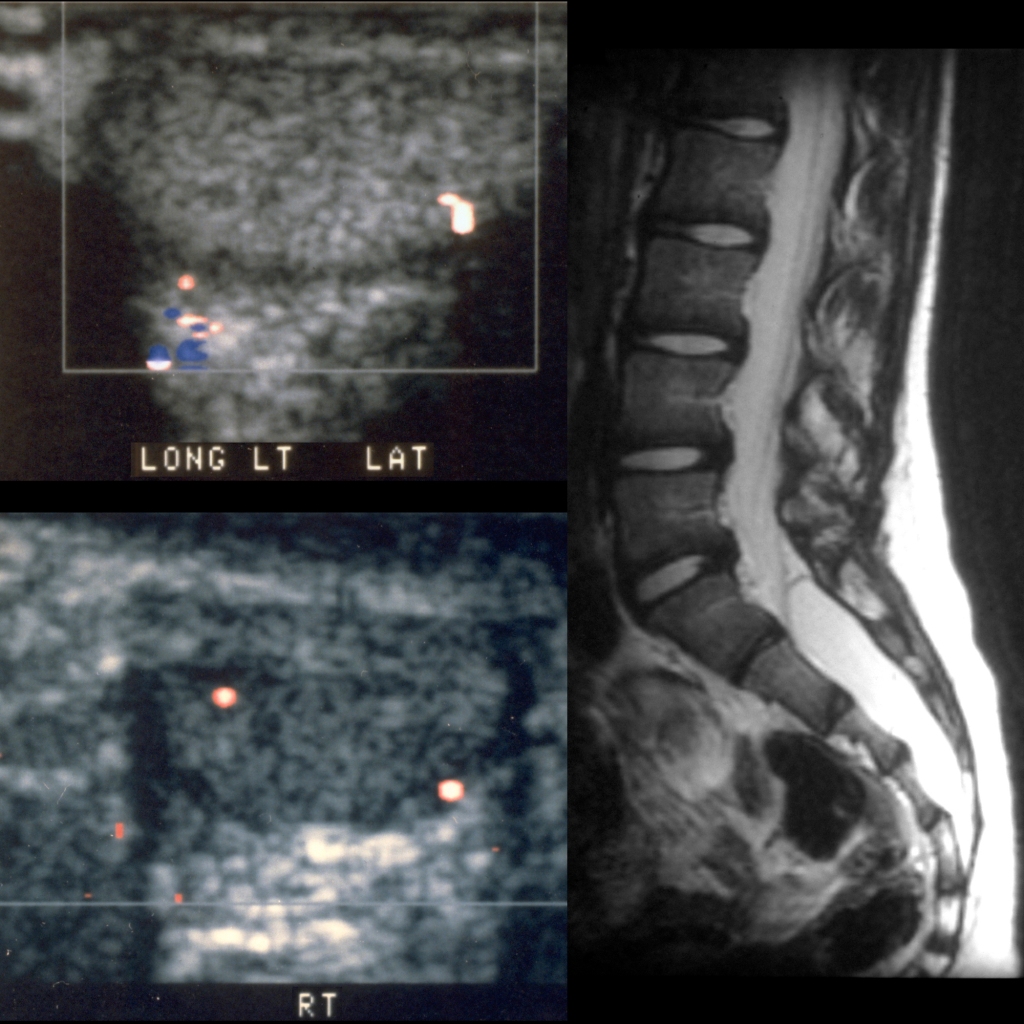
Radiology Cases of Sacral Arachnoid Cyst