
The need for a surgical treatment in a patient with septate uterus depends on the obstetric history rather than the septum and the mainly indication for treatment is a history of reproductive failure. There is still controversy about the indication for metroplasty and while some authors recommend the surgery only in cases of bad obstetrics outcomes, others recommend a prophylactic metroplasty in particular cases.
It is well accepted that the main indication for metroplasty is recurrent pregnancy loss and that the metroplasty significantly improves the reproductive outcomes in patients with septate uterus. The situation remains controversial in women with only one miscarriage and a conservative approach is recommended.
Regarding patients with primary infertility, the role of metroplasty is a matter of debate and other concomitant causes of infertility have to be ruled out. The prospective controlled trial by Mollo found a higher probability of conceiving after removal of the septum compared with patients affected by unexplained infertility.
The role of the hysteroscopy metroplasty in patients that require an assisted reproduction technique is a matter of debate. In a prospective randomized trial on hysteroscopic metroplasty in patients with previous in vitro fertilization (IVF) cycles failure, De Angelis demonstrated the beneficial effects of metroplasty prior to a new IVF cycle in terms of pregnancy rates and in the incidence of miscarriage, concluding that the hysteroscopic metroplasty should be advisable before an IVF cycle to improve the pregnancy rates and to reduce the incidence of spontaneous abortion
In 1974, Edstrom first described the resection of a uterine septum guided by hysteroscopy. This first endoscopic approach was the starting point for the actual metroplasty. Currently, hysteroscopy approach has replaced transabdominal techniques.
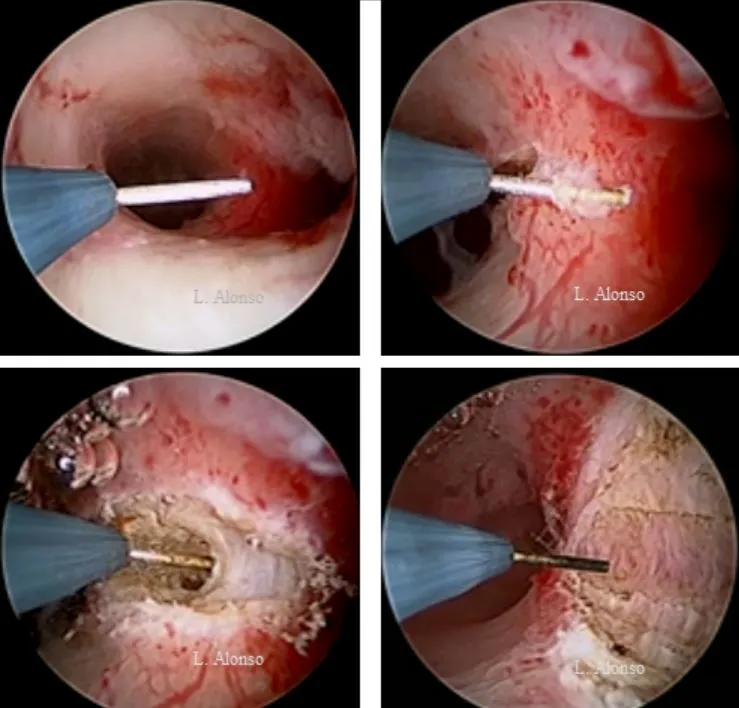
Hysteroscopy metroplasty is, in fact, a transversal incision of the uterine septum instead a resection. This incision has to be made in the middle of the septum, equidistant to the anterior and posterior uterine walls. Tubal ostia are helpful to maintain the right plane avoiding the lesion of the normal myometrium. The determination of the correct incision line is one of the most important parts of the hysteroscopic metroplasty,
but this imaginary line is not always easy to determine. Levent Yasar and Ali Süha Sönmez described the “Süha-Levent sign”. After methylene blue injection, they found a well-defined blue line of 2–3 mm, over the septum between the tubal ostia and equidistant to the anterior and the posterior walls. This blue guide helped them to identify the correct incision line.
Two different surgical approaches for the septum have been described, the thinning technique and the shortening one. In the thinning technique, longitudinal incisions are performed over each side of the uterus from the base to the apex of the septum. The objective is to reduce the width of the septum and to transform the initial septum in a fundical remnant of tissue that can be incised from one cornual recess to the other. In the “shortening” technique, the septum is incised transversely, starting from the apex towards the fundus. This incision in the midline of the septum, retracts the remaining tissue towards the anterior and posterior uterine walls.
The selection of one of the above techniques depends on the width and the length of the septum. As a general recommendation, for a broad septum it is better to use the thinner technique while for a thin septum, the “shortening” is the most appropriate.

0 comments on “Sugical Correction of the Septate Uterus”