History
As previously mentioned, hereditary spastic paraplegia (HSP) is not a single disease entity but a group of clinically and genetically diverse disorders that cause progressive and generally severe lower extremity weakness and spasticity.
Pure, autosomal dominant HSP has been reviewed. After normal gestation, delivery, and early childhood development, subjects develop leg stiffness and gait disturbance (eg, stumbling, tripping) because of difficulty in dorsiflexing the foot and as a result of weakness in hip flexion.
HSP is generally classified as pure or complicated. In pure HSP, symptoms are generally limited to gradual weakening in the legs, urinary bladder disturbance, spasticity, abnormal gait, decreased sense of balance, and, sometimes, impaired sensation in the feet. [6]
In complicated HSP, a rare disorder, additional symptoms may include the following:
-
Peripheral neuropathy
-
Epilepsy
-
Ataxia
-
Optic neuropathy
-
Retinopathy
-
Dementia
-
Ichthyosis
-
Intellectual disability
-
Deafness
-
Problems with speech, swallowing, or breathing
Some of these additional symptoms may be related to a separate disorder, rather than being directly caused by HSP. Patients may actually have pure HSP plus one or more other disorders. For example, a person with pure HSP may have peripheral neuropathy caused by diabetes, or he or she may have unrelated epilepsy.
Additional symptoms
The classic symptom of HSP is progressive difficulty in walking, but the severity varies. Some patients eventually may require the use of a wheelchair, while others may never need any type of assistive device. Patients usually have difficulty lifting their toes; as a result, they drag their toes when walking and catch them on stairs or on uneven sidewalks or curbs. [6]
In later stages, patients experience difficulty flexing the thigh muscle to raise the leg when walking. A reduced sense of balance is noted. Muscles weaken but also experience increased muscle tone. Some patients complain of reduced sensation in the distal regions of the legs.
Some people also experience urinary problems; eg, incontinence or a sense of urgency even when the bladder is not full. [6] A study by Kanavin and Fjermestad found that of 108 adults with hereditary spastic paraplegia (HSP), 30.5% suffered from urinary incontinence at least daily/nightly, while 27.4% needed to urinate more than eight times daily and 51.9% experienced sudden urges to urinate. Moreover, a number of patients reported gastrointestinal problems, including constipation (14.6%), alternation of constipation and diarrhea (8.0%), fecal incontinence (11.6%), an inability to hold back stools (38.5%), and an at least daily occurrence of uncontrollable flatulence (47.6%). [34]
People with HSP also experience hyperactive reflexes. Many symptoms that are common in people with HSP are not directly caused by HSP but are instead caused indirectly by muscle spasticity, weakness, or hyperactive reflexes.
Spasticity
Spasticity is an increase in muscle tone with resulting stiffness. Muscle tone refers to the mild contraction that muscles continue to exhibit even when at rest (ie, resting muscle tone). A reflex between nerve endings in the muscle and spinal cord regulates muscle tone. Normally, the corticospinal nerves control and reduce sensitivity of this reflex. Because HSP causes deterioration of the corticospinal nerves, the reflex is not reduced as it should be, the result being an exaggerated (ie, hyperactive) reflex and increased muscle tone.
Depending on the circumstances, the amount of spasticity experienced is likely to change a good deal. Stiffening of the leg muscles is normal after long periods of sitting, because the muscles have contracted and then are stretched upon standing. Many people also notice that their muscles seem tighter when they are emotionally stressed or upset. Other factors that can affect spasticity are cold temperature, poor posture, high humidity, and illness.
Abnormal gait
Increasing stiffness in the legs is associated with frequent tripping, particularly when the patient is walking on uneven terrain.
Uncontrollable shaking of the legs may be noted when the patient ambulates. Dragging of the feet, scissoring of the legs during ambulation, weakness and giving way at the ankles, flexor spasms of the legs during the night, and a sense of unsteadiness during walking also are common.
Decreased sense of balance
A common symptom of HSP, and often the first one that patients notice, is a decreased sense of balance. Many people with HSP have an impaired sense of foot position. If the brain does not receive accurate signals relating to the body's position, it may not be able to respond properly to those signals, and loss of balance occurs.
Pure HSP kindreds
The age of symptom onset, the rate of symptom progression, and the extent of disability are variable within and between HSP kindreds. In contrast to the extent of disability and to the variable age of patients at symptom onset, the distribution of neurologic deficits in pure HSP is consistent; it consists of spastic weakness in the legs, variable impairment of vibratory sense in the feet, and variable urinary bladder disturbance.
In patients with a pure HSP kindred, the presence of additional deficits, such as visual disturbance, marked muscle wasting, fasciculations, dementia, seizures, and peripheral neuropathy, should not be attributed to variant presentations of pure HSP. Therefore, these patients should be thoroughly evaluated for concurrent or alternative neurologic disorders.
Some pure, autosomal dominant HSP kindreds exhibit an onset of progressive spastic paraplegia in childhood (ie, < P 6y) and relatively little progression of symptoms beyond adolescence. [35] ) These patients often do not experience urinary bladder disturbances generally remain ambulatory with assistance.
Physical Examination
Neurologic examination reveals no evidence of cranial nerve dysfunction or reduced mentation. Although the jaw jerk may be brisk in older subjects, no speech disturbance, difficulty swallowing, or evidence of frank corticobulbar tract dysfunction is noted.
Upper extremity muscle tone and strength are normal. In the lower extremities, muscle tone is increased at the hamstrings, quadriceps, and ankles. Results of manual muscle testing are difficult to assess because of increased tone; however, weakness is occasionally demonstrated in the legs. Weakness is most notable at the iliopsoas muscles, the tibialis anterior muscles, and, to a lesser extent, the hamstring muscles. Muscle wasting may occur in patients with pure HSP, but it is mild and is limited to atrophy of the shins in elderly, wheelchair-dependent patients.
Peripheral nerves are normal in patients with pure HSP, although decreased perception of sharp stimuli below the knees is occasionally noted. Vibratory sensation is often mildly diminished in the distal lower extremities. When it occurs, this deficit provides a diagnostic sign that helps to distinguish HSP from other disorders. Slight terminal dysmetria is occasionally observed on finger-to-nose testing in older affected individuals. Deep tendon reflexes may be brisk (2+ to 3+) in the upper extremities but are pathologically increased (3+ to 4+) in the lower extremities.
The patient's gait demonstrates circumduction owing to a difficulty with hip flexion and ankle dorsiflexion. Crossed adductor reflexes, ankle clonus, and extensor plantar responses are uniformly present. Hoffman and Tromner signs may be observed. High-arched feet (pes cavus) are generally present and are usually prominent in older patients. The photographs seen below depict patients with complicated HSP.
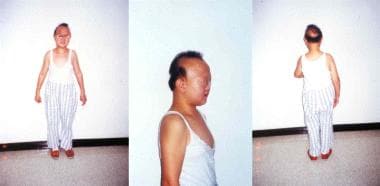 Dysmorphic appearance of a 16-year-old girl with complicated hereditary spastic paraplegia. This patient displays a short stature (145 cm) and hair loss. Anterior (left), lateral (middle), and posterior (right) views are shown.
Dysmorphic appearance of a 16-year-old girl with complicated hereditary spastic paraplegia. This patient displays a short stature (145 cm) and hair loss. Anterior (left), lateral (middle), and posterior (right) views are shown.
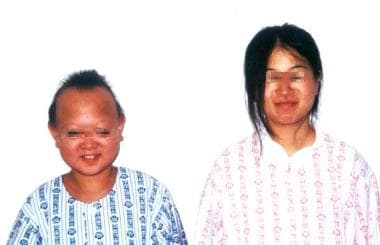 General appearance of sisters with complicated hereditary spastic paraplegia. They are aged 16 and 17 years. Physical examination revealed increased deep tendon reflexes in all 4 extremities, with an extensor plantar reflex. Sensory losses in the patients have affected mainly their joint positions and vibration sensations.
General appearance of sisters with complicated hereditary spastic paraplegia. They are aged 16 and 17 years. Physical examination revealed increased deep tendon reflexes in all 4 extremities, with an extensor plantar reflex. Sensory losses in the patients have affected mainly their joint positions and vibration sensations.
-
Photograph of a 16-year-old girl with complicated hereditary spastic paraplegia. She has a spastic gait disturbance, intellectual disability, and extrapyramidal symptoms. Note the dysmorphic features.
-
Dysmorphic appearance of a 16-year-old girl with complicated hereditary spastic paraplegia. This patient displays a short stature (145 cm) and hair loss. Anterior (left), lateral (middle), and posterior (right) views are shown.
-
General appearance of sisters with complicated hereditary spastic paraplegia. They are aged 16 and 17 years. Physical examination revealed increased deep tendon reflexes in all 4 extremities, with an extensor plantar reflex. Sensory losses in the patients have affected mainly their joint positions and vibration sensations.







