Medical Therapy
Observation is indicated in most hemangiomas. Presentation of images showing the natural course of hemangiomas is very useful when discussing the natural course of the disease with parents and/or caregivers. [23] However, 40% of hemangiomas that have completed the involution phase leave significant disfigurement that may necessitate late intervention. [4, 15]
Nonsurgical therapy is discussed below.
Local wound care
Local antibiotic ointment or wet-to-dry dressing is useful to clear the debris and decrease the likelihood of local infection during the involution stage when the lesion becomes ulcerated. Parents need to be informed about the possibility of acute bleeding and how to apply local pressure.
Local pressure
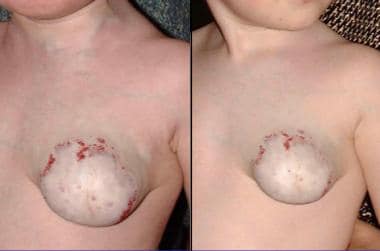
Wearing a pressure garment for at least 20 hours every day may be helpful in suitable anatomic sites. [24] The image below shows the effect of a pressure garment on a large chest hemangioma. The lesion decreased following treatment of this 1-year-old girl with a compression garment 20 hours every day for 4 months. Local excision was deferred to avoid injury to the breast bud.
Propranolol
Although propranolol has rapidly been adopted, there is significant uncertainty and divergence of opinion regarding safety monitoring, dose escalation, and its use in PHACE syndrome. [25] Because of the absence of high-quality clinical research data, evidence-based recommendations are not possible at present.
A study by Li et al suggested that propranolol may cause regression of infantile hemangioma by suppressing the signaling pathways of vascular endothelial growth factor (VEGF) and the oncogenic signaling molecule signal transducer and activator of transcription 3 (STAT3). The study also indicated that this suppression is dependent on hypoxia inducible factor-1 α (HIF-1 α). [26]
Steroids
Systemic or local injection of steroids is indicated in certain patients during the growth phase. [9, 10] The usual dosage is up to 2-3 mg/kg/d for 4-6 weeks with gradual tapering of the dosage afterwards. The dosage may be increased up to 5 mg/kg/d in severe cases. Steroid treatment is indicated when major functional complications arise. Among the patients treated with steroids, one third have very satisfactory results, one third show partial or temporary reduction in mass, and the remainder demonstrate minimal or no response to treatment. Pope showed that oral corticosteroids offer more clinical and biological benefit than intravenous pulse steroids. [27]
The image below shows the effect of local and systemic steroid treatment on orbital hemangioma. The 9-month-old infant girl in the image was able to open her eye again following 3 months of treatment.

Short-term adverse effects that are minor and transient may occur. Long-term complications are uncommon. [28]
Recombinant interferon alfa-2a
Recombinant interferon alfa-2a may be indicated in patients in whom steroids are contraindicated or not effective. [11] Treatment is associated with complications such as transient elevation of liver enzyme levels, neutropenia, and anemia. A concerning complication is the possibility of long-term spastic diplegia. [15] Recently, vincristine has been suggested as an alternative treatment for corticosteroid-resistant hemangiomas. [29]
Flash lamp pulsed dye laser
This device has a moderate lightening effect on the capillary discoloration of hemangiomas. Pulsed dye laser does not have an effect on the volume of the lesions. [30]
Intralesional laser
An intralesional fiber with the potassium-titanyl-phosphate (KTP) laser was demonstrated to induce involution of voluminous hemangiomas of the face and neck regions. [12, 13] Intralesional photocoagulation treatment with the KTP and Nd:YAG lasers was also found to be effective and safe for the treatment of periorbital hemangiomas. [14]
Carbon dioxide laser
This tool is useful for treating subglottic hemangiomas. It may also be useful for resurfacing residual minor skin irregularities.
Superselective catheterization and embolization
This is infrequently used to treat hemangiomas with a defined nourishing artery. Embolization may be useful to decrease high-output cardiac failure in infants with liver hemangiomas.
Surgical Therapy
Surgical therapy may be considered in several circumstances, including the following:
-
When intraoperative and postoperative bleeding can be controlled
-
When surgery does not place an organ at risk (eg, injury to the eye or facial nerve)
-
When the expected aesthetic and/or functional outcomes of the procedure are similar to or superior to the aesthetic outcome of spontaneous involution
-
When the aesthetic and/or functional outcomes of the procedure are inferior to the predicted outcome of spontaneous involution and the psychosocial effect on the child having to live through childhood with a disfiguring deformity is significant
Regional approach to the management of facial hemangiomas
Facial hemangiomas are a challenge. They are associated with significant parental concerns and psychosocial effect on the developing child. A regional approach to the management of those often very disfiguring lesions is discussed below.
Periorbital hemangiomas
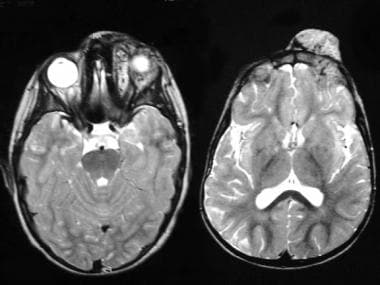
Most hemangiomas in this area are managed by a conservative approach (see the images below). Treatment with local injections and/or systemic steroids is indicated when vision is impaired and such impairment may cause astigmatism or deprivation amblyopia (see the first image below). Late excision may be indicated for residual fibrous fatty tissue. MRI is mandatory to exclude other benign or malignant causes of periorbital fullness, proptosis, and dystopia. The differential diagnosis (see the fourth image below) includes lymphatic lesions, neurofibromatosis, meningioma, lacrimal epithelial tumors, and fibrous dysplasia.

Forehead hemangiomas
The combination of a relatively thin skin, subcutaneous tissue, and muscle causes most forehead hemangiomas to become exophytic (see the images below). These lesions, especially when located close to or within the hairline, tend to bleed profusely. This may require early resection (see the first image below). Lower forehead hemangiomas may cause secondary ptosis. The lesions can be excised through a direct incision. A bicoronal approach provides excellent exposure and allows wide resection of the lesion without visible scars.


The image above demonstrates resection of a lower forehead hemangioma at the fibrous fatty stage through a bicoronal approach. The lesion (upper left and middle images) was exposed through a bicoronal incision (upper right) and excised (lower left). The nasal bridge was exposed and excess fibrofatty tissue was resected as well (lower middle). A satisfactory result is observed 3 months after surgery (lower right).
Cheek hemangiomas
Most hemangiomas in this area are managed by a conservative approach. Systemic and/or local treatment with steroids is indicated when vision is impaired. The aesthetic outcome of deep lesions is excellent. The first image below demonstrates 2 patients, one aged 1 year and one aged 8 years, with deep cheek hemangiomas. An excellent outcome with conservative treatment is shown. When the hemangioma includes a superficial skin involvement, future intervention to address excess skin and skin texture is anticipated. The second image below shows 2 patients who had cheek hemangiomas with a superficial component. The patient in the upper part of the figure is observed at age 9 months and age 9 years. The patient in the lower part of the image is observed at age 4 months and age 5 years.


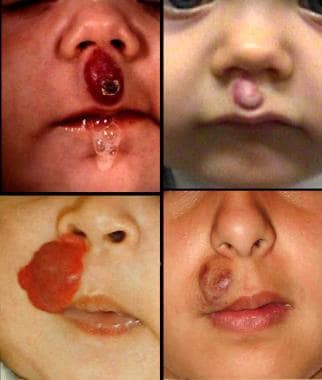
Nasal hemangiomas
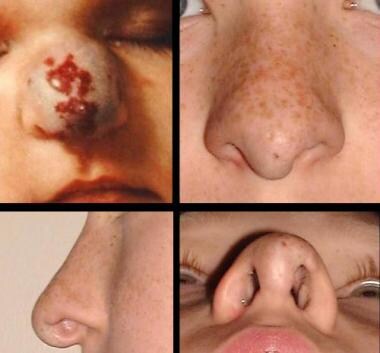
Based on their location, hemangiomas can be classified (see the image below) into nasal tip lesions, nasal bridge lesions, and lateral nasal lesions. Lateral nasal lesions are managed in the same manner as cheek lesions, and early treatment of those lesions with steroids is indicated when vision is obstructed.

In the authors' experience, early surgery has proved to be beneficial for nasal bridge and nasal tip lesions. The feasibility of the surgical intervention depends on the size of the lesion and the likelihood of aesthetically pleasing primary skin closure. The surgical excision can be preceded by local steroid injections. Nasal bridge lesions can be excised and the skin primarily closed in many patients. Nasal tip ("Pinocchio") lesions can be addressed by open rhinoplasty when the individual is aged 3-4 years. The vascular lesion is excised from the inner side of the nasal skin. The tip is redraped and the excess skin is excised. The second image below shows the outcome of early excision of a nasal tip hemangioma (upper left). The nose is observed (lower left; upper and lower right) 10 years following open rhinoplasty performed when the patient was aged 2.5 years.

Upper lip hemangiomas
Upper lip hemangiomas are usually not associated with functional problems. They are associated with aesthetic concerns and cause discoloration, protrusion, and lip ptosis on the affected side due to their mass effect. [31] In the authors' experience, lesions that do not involve the skin can be excised through an intraoral approach with good aesthetic outcome. Lesions that involve the skin are best managed conservatively until the lesion decreases. Waiting allows reconstruction of the entire aesthetic unit or subunit of the upper lip. This usually makes an almost impossible reconstruction a feasible one.
The image below shows the natural course of upper lip lesions that involve the skin. The upper and lower left images show upper lip hemangiomas in individuals aged 9 months and 2 years, respectively. The upper and lower right images show upper lip hemangioma in individuals aged 6 years and 11 years, respectively. Observation facilitates lip reconstruction but may be associated with a severe psychosocial effect on the child. This should always be taken into consideration when surgery is planned. The girl observed in the lower left and right pictures was frequently teased by her peers because of the "worm" on her upper lip.
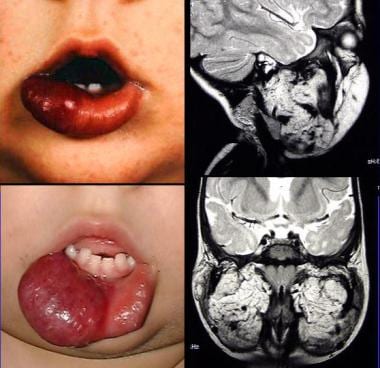
Lower lip hemangiomas
Lower lip lesions have aesthetic as well as functional consequences. [32] Lip protrusion and ptosis may cause drooling and speech impairment (see the first image below). The lesions may extend into the floor of the mouth. The visible lip lesion in these patients is usually the "tip of an iceberg." The second image below shows a lower lip hemangioma in an individual at age 6 months (upper left) and following proliferation at age 16 months (lower left). MRI shows involvement of the floor of the mouth and cheek. Lip reduction is advised in such patients at the end of the proliferation phase. This can be performed by a fusiform mucosal excision with lip debulking. Tumescence is a valuable adjunct for the excision of such lesions. [33]

Rapidly spreading panfacial hemangiomas
The authors define rapidly spreading "malignant"-type hemangiomas as lesions that quickly extend from their original aesthetic units. These lesions frequently are associated with significant aesthetic deformities. They require early detection and treatment with steroids. The healing process may be associated with necrosis and soft tissue loss that produce severe facial deformities.
The image below, upper left, shows a 4-month-old infant girl with rapidly spreading hemangioma that started as a small cheek nodule and eventually invaded the forehead, eyelids, cheek, and lip aesthetic units. Part of the lip underwent necrosis and caused a cleft of the lip (lower left). The images on the right are of 6-month-old (upper right) and 4-month-old (lower right) infants with aggressive, rapidly spreading hemangiomas. Parents need to be informed that administration of steroids may induce repulsive necrosis of the lesion. See the image below, lower right.

Complications
Vision
Obstruction of vision during the first 6 months of life by a periorbital, cheek, forehead, or nasal hemangioma may cause long-term visual damage. Early treatment with steroids, surgery, or both is indicated in such patients.
Breathing
Hemangiomas that invade the neck may compress the soft tracheal rings of infants and present as stridor. Steroids are indicated in these patients. Direct external excision of the lesions is impossible in most patients because of close proximity of the hemangioma to vital structures. Localized subglottic lesions can be reopened with carbon dioxide laser. Consider tracheostomy for patients who have failed to improve from pharmacologic treatment.
Bleeding
Hemangiomas have a high flow during the proliferative phase, and when extensive lesions become ulcerated, anemia may result. This is especially common in the scalp. Parents are instructed to apply pressure over the bleeding area. Pharmacologic treatment and/or surgery are indicated for symptomatic patients. The image below shows a small but repeatedly bleeding forehead hemangioma before and after surgical excision.
Thrombocytopenia
Large hemangiomas with a high flow may be associated with platelet trapping and thrombocytopenia (Kasabach-Merritt phenomenon). Pharmacologic treatment is indicated in such patients.
Psychosocial complications
Many facial hemangiomas cause a significant facial deformity during the proliferative and early involution phases. Facial appearance usually improves when the individual is older than 10 years. [15] Children with facial hemangiomas are often teased by their peers. Early surgery may be indicated in such situations.
Outcome and Prognosis
Most hemangiomas appear during the first months of life, undergo proliferation with a peak at age 1 year, and then undergo gradual involution. Involution is 50% complete by age 5 years and 70% complete by age 7 years, with continued improvement up to age 10-12 years. [15] An exception is congenital hemangioma, which is present at birth and usually undergoes regression at approximately age 1 year. [15] Noninvoluting congenital hemangioma is a variant of the common hemangioma of infancy with persistent fast flow. [34] Unlike vascular malformations, hemangiomas rarely cause bony distortion and overgrowth, with the exception of huge facial hemangiomas, which may affect the underlying bone and cartilage. [15, 35]
A study by Rialon et al indicated that the risk of mortality in patients with hepatic hemangioma is greater in those with CHF and in patients with diffuse, rather than multifocal, lesions. The study involved 123 patients with either the multifocal or diffuse form of the condition. [36]
In a retrospective, single-center, case-control study of patients with congenital hepatic hemangiomas, Delgado-Miguel et al found that in those who died as a result of cardiac failure and coagulopathy, median liver enzyme concentrations were significantly higher than in those who survived (glutamic-oxaloacetic transaminase levels of 359 u/L vs 45 u/L, respectively, and glutamic-pyruvic transaminase levels of 313 u/L vs 20 u/L, respectively). Moreover, the median platelet count was reduced in non-survivors (85,250/µL vs 337,000/µL), as was prothrombin activity and the fibrinogen level. [37]
Various associated medical conditions are discussed in Physical examination.
Future and Controversies
The introduction of a classification method by Mulliken and associates was a significant contribution to the understanding of vascular legions. [1] This made diagnosis and treatment more accurate and predictable. However, confusing and occasionally wrong terms used by different subspecialties are still found.
Improvement in patient monitoring and anesthesia during and after surgery made early excisions safer and more acceptable. Other contributions included the introduction of the pulsed dye laser, which helps fade away the capillary component of hemangiomas, [30] and the intralesional fiber laser. [12, 33]
A major controversy is whether to wait until involution is complete or to operate early on children with disfiguring lesions. No clear-cut answer exists to this question. The authors believe that decisions should be made according to the individual situation. The psychosocial consequences of growing up with a facial deformity should always be taken into consideration.
Future genetic research, including angiogenic growth factor products, will contribute to the understanding of the mechanism underlying the formation of hemangiomas and may provide new modalities for treatment. [17] Because bFGF and VEGF messenger RNA have been implicated in the pathobiology of human hemangioma formation, biochemical modulation of these angiogenic cytokines may eventually help inhibit proliferation and promote regression of hemangiomas. [19]
-
Hemangiomas. Classification of vascular lesions.
-
Hemangiomas. Classification of vascular malformations.
-
Hemangiomas. Diagnosis - Medical history.
-
Hemangiomas. Diagnosis - Physical examination.
-
Deep cheek hemangiomas.
-
Superficial cheek hemangiomas.
-
Upper lip hemangiomas.
-
Treatment with steroids of orbital hemangioma.
-
Panfacial hemangiomas.
-
Resection of a bleeding forehead hemangioma.
-
Lower lip hemangioma with intraoral extension.
-
Hemangiomas. Relaxation time - MRI T1, T2.
-
Hemangiomas. Diagnosis MRI.
-
Left orbital hemangioma.
-
MRI of orbital hemangioma.
-
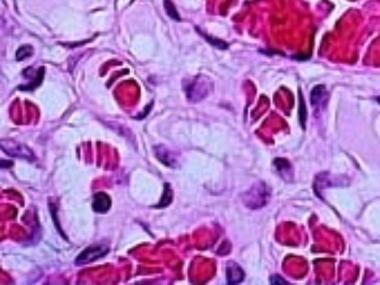
Proliferating hemangioma - Light microscopy.
-
Hemangiomas. Facial nodular fasciitis misdiagnosed as a vascular lesion.
-
Differential diagnosis of orbital hemangiomas.
-
The effect of compression on a chest hemangioma.
-
Use of a bicoronal approach to resect a forehead hemangioma.
-
Types of nasal hemangiomas.
-
Resection and primary closure of a nasal bridge hemangioma.
-
Open rhinoplasty approach to resect a nasal tip hemangioma.
-
Lower lip hemangioma.





