History
Patients with Charcot-Marie-Tooth (CMT) disease have a significant family history. This history varies depending on the inheritance and penetrance pattern of the particular disorder (see Etiology). Spontaneous mutations also have been reported.
The age of presentation varies, depending on the type of CMT disease. Onset usually occurs in the first two decades of life.
Slowly progressing weakness beginning in the distal limb muscles is generally noted; it typically occurs in the lower extremities before it affects the upper ones. A subgroup of patients with CMT 1A may present with proximal muscle wasting and weakness.
Patients initially may complain of difficulty walking and frequent tripping due to foot and distal leg weakness. Frequent ankle sprains and falls are characteristic. Parents may report that a child is clumsy or simply not very athletic. As weakness becomes more severe, foot drop commonly occurs. Steppage (that is, gait in which the individual must lift the leg in an exaggerated fashion to clear the foot off of the ground) also is common.
Intrinsic foot muscle weakness commonly results in the foot deformity known as pes cavus. [38] Symptoms related to structural foot abnormalities include calluses, ulcers, cellulitis, and lymphangitis.
Hand weakness results in complaints of poor finger control, poor handwriting, difficulty using zippers and buttons, and clumsiness in manipulating small objects. Multidisciplinary assessment is warranted for evaluating impairment of manual function. [39] The hand may be affected at all ages in children with CMT 1A; hand problems in these patients may be underrecognized in the early stages of disease, causing potential delay in therapy. [40]
Patients usually do not complain of numbness. This may be because patients with CMT disease never had normal sensation and, therefore, simply do not perceive their lack of sensation.
Pain (musculoskeletal and neuropathic types) may be present. Muscle cramping is a common complaint. [41]
Autonomic symptoms usually are absent, but a few men with CMT disease have reported impotence.
Physical Examination
Distal muscle wasting may be noted in the legs, resulting in the characteristic stork leg or inverted champagne bottle appearance.
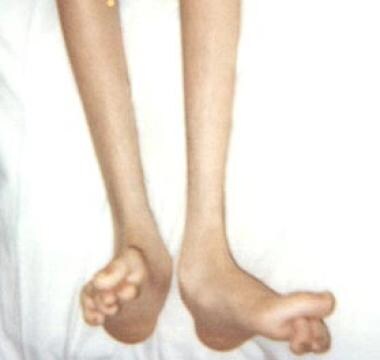
Bony abnormalities commonly seen in long-standing CMT disease include pes cavus (high-arch foot), probably analogous to the development of claw hand in ulnar nerve lesions. Pes cavus has an occurrence rate of 25% in the first decade of life and 67% in later decades. Selective denervation of intrinsic foot musculature (particularly of the lumbricals), rather than imbalance of lower-leg muscles, seems to be the initial mechanism causing reduced ankle flexibility and forefoot cavus deformity. [42] Other foot deformities also can occur (see the image below). Charcot joints may develop. [43]
Spinal deformities (eg, thoracic scoliosis) occur in 37-50% of patients with CMT 1.
Deep tendon reflexes (DTRs) are markedly diminished or are absent. Vibration sensation and proprioception are significantly decreased, but patients usually have no sensory symptoms.
Patients may have sensory gait ataxia, and a Romberg test usually yields positive results. The Romberg test is performed by having the patient stand upright with the feet together and the eyes closed. The examiner observes the patient's body movement relative to a perpendicular object behind him or her (eg, a door or window). Pronounced, sometimes irregular swaying, or occasionally even toppling over, constitutes a positive result. The key point is that the patient's unsteadiness increases when his or her eyes are closed.
Impairment of vestibular function, as measured by the video head impulse test (vHIT), may be reflected in worse postural balance, as measured by postural tests such as the modified clinical test of sensory integration in balance (mCTSIB). [44]
Sensation of pain and temperature is usually intact. Essential tremor is present in 30-50% of patients with CMT disease. Sensory neuronal hearing loss is observed in 5% of patients. Enlarged and palpable peripheral nerves are common. Phrenic nerve involvement with diaphragmatic weakness is rare but has been described. Vocal cord involvement and hearing loss can occur in rare forms of CMT disease.
Complications
Because of the loss of protective sensation distally in all four limbs, patients with CMT disease are susceptible to skin breakdown or burns, nonhealing foot ulcers, and, in severe cases, bony deformities of bilateral feet. As mentioned previously, orthoses are required for treatment of foot drop or to accommodate bony foot deformities. If not fitted properly, the orthoses themselves become a source of skin breakdown secondary to associated distal sensory impairment.
The presence of maternal CMT disease is associated with an increased risk of complications during delivery. This increase is related to a higher frequency of emergency interventions during birth. [36]
-
Foot deformities in 16-year-old boy with Charcot-Marie-Tooth disease type 1A.
-
Charcot-Marie-Tooth disease type 1A DNA test showing duplication in short arm of chromosome 17 (A); compared with normal (B).
-
Nerve conduction study showing decreased nerve conduction velocity in median nerve in 18-year-old woman with Charcot-Marie-Tooth disease type 1.
-
Cavovarus feet with heels visible from front ("peekaboo" sign).
-
High arch typical of patients with cavus feet.
-
Both heels showing varus deformity when observed from back.
-
Coleman block test showing lack of correction of hindfoot varus malalignment when block is placed under outer border of foot.
Tables
CMT Type |
Chromosome; Inheritance Pattern |
Age of Onset |
Clinical Features |
Average NCVs§ |
CMT 1A (PMP-22¶ dupl.) |
17p11; AD* |
First decade |
Distal weakness |
15-20 m/s |
CMT 1B (P0 -MPZ)** |
1q22; AD |
First decade |
Distal weakness |
< 20 m/s |
CMT 1C (non A, non B) |
16p13;AD |
Second decade |
Distal weakness |
26-42 m/s |
10q21; AD |
First decade |
Distal weakness |
15-20 m/s |
|
CMT 1E |
17p11; AD |
First decade |
Distal weakness, deafness |
15-20 m/s |
CMT 1F |
8p21; AD |
First decade |
Distal weakness |
15-20 m/s |
Xq13; XD‡ |
Second decade |
Distal weakness |
25-40 m/s |
|
CMT 2A |
1p36; AD |
10 y |
Distal weakness |
>38 m/s |
CMT 2B |
3q; AD |
Second decade |
Distal weakness, sensory loss, skin ulcers |
Axon loss; Normal |
CMT 2C |
12q23-q24, AD |
First decade |
Vocal cord, diaphragm, and distal weakness |
>50 m/s |
CMT 2D |
7p14; AD |
16-30 y |
Distal weakness, upper limb predominantly |
Axon loss; N†† |
CMT 2E |
8p21; AD |
10-30 y |
Distal weakness, lower limb predominantly |
Axon loss; N |
CMT 2F |
7q11-q21; AD |
15-25 y |
Distal weakness |
Axon loss; N |
CMT 2G |
12q12-q13; ?AD |
9-76 y |
Distal weakness |
Axon loss; N |
CMT 2H |
?; AR† |
15-25 y |
Distal weakness, pyramidal features |
Axon loss; N |
CMT 2I |
1q22; AD |
47-60 y |
Distal weakness |
Axon loss; N |
CMT 2J |
1q22; AD |
40-50 y |
Distal weakness, hearing loss |
Axon loss; N |
CMT 2K |
8q13-q21; AR |
< 4 y |
Distal weakness |
Axon loss; N |
CMT 2L |
12q24; AD |
15-25 y |
Distal weakness |
Axon loss; N |
CMT R-Ax (Ouvrier) |
AR |
First decade |
Distal weakness |
Axon loss; N |
CMT R-Ax (Moroccan) |
1q21; AR |
Second decade |
Distal weakness |
Axon loss; N |
Cowchock syndrome |
Xq24-q26 |
First decade |
Distal weakness, deafness, intellectual disability |
Axon loss; N |
HNPP|| (PMP-22) Or tomaculous neuropathy |
17p11; AD |
All ages |
Episodic weakness and numbness |
Conduction Blocks |
Dejerine-Sottas syndrome (DSS) or hereditary motor and sensory neuropathy (HMSN) 3 |
P0; AR PMP-22; AD 8q23; AD |
2 y |
Severe weakness |
< 10 m/s |
Congenital hypomyelination (CH) |
P0, EGR2 or PMP-22 AR |
Birth |
Severe weakness |
< 10 m/s |
CMT 4A |
8q13; AR |
Childhood |
Distal weakness |
Slow |
CMT 4B (Myotubular in-related protein-2) [18] |
11q23; AR |
2-4 y |
Distal and proximal weakness |
Slow |
CMT 4C |
5q23; AR |
5-15 y |
Delayed walking |
14-32 m/s |
CMT 4D (Lom) (N-myc Downstream- Regulated Gene 1) |
8q24; AR |
1-10 y |
Distal muscle wasting, foot and hand deformities |
10-20 m/s |
CMT 4E (EGR2) |
10q21; AR |
Birth |
Infant hypotonia |
9-20 m/s |
CMT 4G |
10q23.2; AR |
8-16 years |
Distal weakness |
9-20 m/s |
CMT 4H |
12p11.21-q13.11; AR |
0-2 years |
Delayed walking |
9-20 m/s |
CMT 4F |
19q13; AR |
1-3 y |
Motor delay |
Absent |
*Autosomal dominant †Autosomal recessive ‡X-linked dominant §Nerve conduction velocities ||Hereditary neuropathy with liability to pressure palsy ¶Peripheral myelin protein #Early growth response **Myelin protein zero ††Normal |
||||







