History
Degos disease, also known as malignant atrophic papulosis or Kohlmeier-Degos disease, is a rare disorder resulting from a vasculopathy, which can affect the skin, gastrointestinal tract, and CNS. [17] The pathognomonic skin lesions have a porcelain-white atrophic center and erythematous telangiectatic rim. Although the disease can affect patients of any age, it typically presents between the second and fifth decades of life. [17] One study by Theodoridis et al [10] described a mean age of onset of 35.4 years (± 12.3 years), with a female-to-male ratio of 1.4:1.
Prognosis is primarily determined by the existence of systemic involvement. [10] A 2018 study by Hu et al described a median of 2 years after diagnosis of Degos disease to the presentation of other systemic symptoms. [24] In this study, the gastrointestinal tract was involved in 82.7% of patients and the CNS in 42.3%.
Patients with Degos disease may note abdominal, neurological, ophthalmological, or pulmonary complaints, including abdominal pain, abdominal distention, cramps, nausea, vomiting, diarrhea, constipation, facial and acral paresthesia, headaches, dizziness, seizures, hemiplegia, aphasia, paraplegia, gaze palsy, diplopia, ptosis, visual-field defects, weakness, shortness of breath, and chest pain. It is important to obtain a proper review of systems, and positive findings should elicit further investigation and workup.
Familial Degos disease has been reported in several cases. In 1997, Katz et al [25] described a familial variant of Degos disease. Theodoridis et al noted familial occurrence in 9% of cases in their study. [10]
Degos disease has been associated with systemic diseases. Degos disease has occurred in patients with rheumatoid arthritis, HIV infection, and antiphospholipid antibodies and antiphospholipid syndrome. [26] Degos disease associated with a spontaneous cure of diabetes has been reported. [27] A case of Degos disease occurring with diabetes mellitus, with biopsy findings of both Degos disease and hyaline diabetic microangiopathy, has also been reported. [28]
Several cases have been reported during pregnancy or in the peripartum period. A case of Degos disease developing during early pregnancy resulting in induction of labor, with biopsy findings consistent with Degos disease with ischemic gastrointestinal complications, has been reported. [29] Hu et al [24] described a case of malignant atrophic papulosis with subsequent motor aphasia and intestinal perforation in a women 10 days after delivery of a full-term pregnancy. A benign variant developing during pregnancy has also been described. [30]
Degos disease has been described in the setting of several infections. Parvovirus B19–associated catastrophic endothelialitis with a Degos-like presentation has been noted. [31] Poststreptococcal vasculopathy that evolved into Degos disease–like white papules has been reported. [32]
Ortiz et al reported a case of cutaneous Degos disease that showed features of connective-tissue disease; a specific connective-tissue disease never developed in the patient. [33] Saglik et al [34] noted a case of malignant atrophic papulosis with endocardial involvement and positive anticardiolipin antibodies.
Physical Examination
Degos disease typically manifests with multiple, small, red, raised papules that are 2-5 mm in diameter. After a few days, they enlarge and develop a central porcelain-white atrophic appearance that is depressed in comparison to the erythematous rim, as shown in the images below. They heal, leaving depressed porcelain white scars with a rim of telangiectases. These erythematous papules with a white atrophic center, characterized as a crown of thorns, are reportedly pathognomonic of Degos disease. [35]
Lesions favor the trunk and upper extremities, but they can also be found on the penis. [36] Involvement of palms and soles and is uncommon. [36] One case has noted that Degos lesions occurred on the scalp. No cases known to the authors note Degos disease-type papules on the face.
 Four papules of Degos disease located on upper-inner arm in different stages of evolution. Courtesy of David F. Butler, MD.
Four papules of Degos disease located on upper-inner arm in different stages of evolution. Courtesy of David F. Butler, MD.
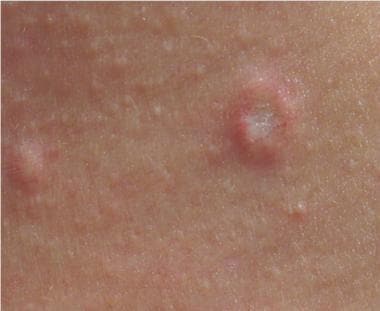 Papule of Degos disease with central sclerosis and telangiectasia. Courtesy of David F. Butler, MD.
Papule of Degos disease with central sclerosis and telangiectasia. Courtesy of David F. Butler, MD.
A full physical examination should be performed, given the risks of systemic involvement, including an ophthalmologic examination, palpation, percussion and auscultation of the abdomen, auscultation of heart and lungs, and a neurologic examination.
A variety of ocular findings occur in Degos disease. Posterior subcapsular cataracts, [37] visual-field defects, ptosis, third cranial nerve palsies, blepharoptosis, and optic atrophy may be associated with Degos disease. Optical neuritis, papilledema, and scleral plaques can be present. [38] In 1986, Sibillat et al [39] reported that ophthalmologic symptoms were present in 35 of 105 extant reports of Degos disease. Degos disease manifested in the eye tissues, usually in the conjunctiva. The sclera, the episclera, the retina, the choroid, the optic nerve, and/or the neuro-ophthalmologic apparatus demonstrated damage consonant with Degos disease.
Patients experience abdominal pain. Gastrointestinal bleeding can result in vomiting blood or passing blood with bowel movements. Patients with Degos disease may have enterocutaneous fistulae.
Complications
The most common organ systems affected are the CNS and gastrointestinal tract. [24] The most frequent causes of death include cerebral infarction, intestinal perforation, and secondary peritonitis. [24]
Complications of Degos disease include the following:
-
Gastrointestinal infarcts, bleeding, and perforation
-
Cardiac pathologic conditions, including pericardial effusions, possible pericardial thickening, and constrictive pericarditis [41]
-
Pulmonary pathologic conditions, including pleuritis and pulmonary effusions
-
Four papules of Degos disease located on upper-inner arm in different stages of evolution. Courtesy of David F. Butler, MD.
-
Papule of Degos disease with central sclerosis and telangiectasia. Courtesy of David F. Butler, MD.
-
Superficial and mid-dermal perivascular lymphocytic infiltrate with focal vacuolar change at the dermoepidermal junction (hematoxylin and eosin, X100). Courtesy of David F. Butler, MD.
-
Alcian blue stain for mucin (X100). Courtesy of David F. Butler, MD.
-
Wedge-shaped area of dermal sclerosis (hematoxylin and eosin, X100). Courtesy of David F. Butler, MD.







